
Prospective Randomized Studies and Meta-analyses of Intervention Studies
Results of the DOPPS study, in line with previous clinical reports, have stimulated interest for HDF and triggered five European interventional prospective randomized controlled trials (RCTs) (1).
The first study to be reported was the Dutch CONvective TRAnsport STudy (CONTRAST). In this prospective study, 714 chronic hemodialysis Dutch and Canadian patients were assigned to either start online postdilution hemodiafiltration (HDF) (n=358) or to continue low-flux HD (n=356) (2,3). A median substitution volume of 19.8 L/session (mean 20.7 L/session) was delivered overall. The primary outcome measure was all-cause mortality, and the main secondary endpoint was a composite of major cardiovascular events. After a mean follow-up of three years, there was no significant difference between treatment groups with regard to all-cause mortality or cardiovascular events. However, in a post hoc analysis considering convection volume, patients receiving high-volume HDF (>21.95 L/session) were associated with lower all-cause mortality compared to the low-flux HD group, a finding that persisted after adjusting for potential confounders and dialysis facility (Figure 1). The strengths of the study are its randomized design and the accuracy of monitoring and data collection. The main limitations of the study are that 9% of the HDF treatments were delivered as high-flux hemodialysis and the lack of compliance to assigned convection volume (6L/hr.; 24L/session) in about two-thirds of HDF-treated patients (4-6).
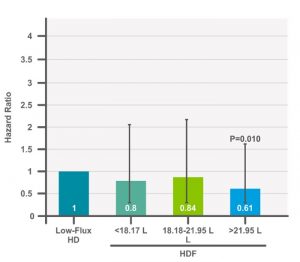
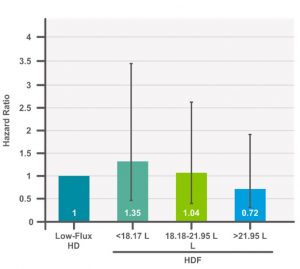
Figure 1. Adjusted all-cause and cardiovascular mortality in LF-HD vs. HDF (3).
The second study was the Turkish HDF study (THDF study). The aim of the THDF study was to compare post dilution online HDF and high-flux HD in terms of morbidity and mortality (7). This prospective, randomized, controlled trial enrolled 782 patients undergoing thrice-weekly HD and randomly assigned them in a 1:1 ratio. The mean follow-up period was 22.7 ± 10.9 months. The primary outcome was a composite of death from any cause and nonfatal cardiovascular events. The mean substitution volume delivered in HDF was 17.2 ± 1.3 liters. The primary outcome was not different between nor were the secondary outcomes of cardiovascular and overall survival. In a post hoc analysis, the subgroup of HDF patients treated with a median substitution volume > 17.4 L/session (equivalent to convection volume of 20.5 L/session) had significantly better cardiovascular and overall survival compared with the high-flux HD group (Figure 2). In adjusted Cox-regression analysis, treatment with high-efficiency HDF was associated with a 46% risk reduction for overall mortality and a 71% risk reduction for cardiovascular mortality compared with high-flux HD. The study had additional limitations that included the fact that enrolled patients were prevalent, relatively young with low comorbid profiles, and particularly well-treated patients (i.e., 90% had blood pressure control without medication and AV fistula).
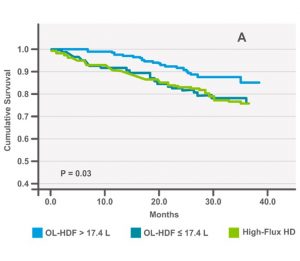
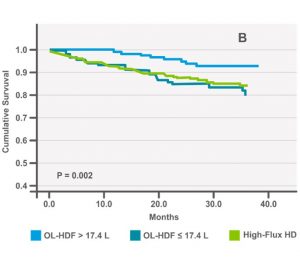
Figure 2. Increased overall (A) and cardiovascular (B) survival in patients treated with a median substitution volume > 17.4 L/session (7) (p. 199).
The third study to be reported was the ESHOL (Estudio de Super-vivencia de Hemodiafiltración On-Line) study. This was a Spanish multicenter, open-label, randomized controlled trial involving 906 prevalent patients (8). In this study, patients were assigned either to continue high flux HD (n=450) or switch to high-efficiency postdilution online HDF (n=456). The median convection volume ranged between 22.9–23.9 L/session in HDF patients. The primary outcome was all-cause mortality, and secondary outcomes included cardiovascular mortality, all-cause hospitalization, treatment tolerability, and laboratory data. HDF–treated patients had a 30% lower risk of all-cause mortality (Figure 3), a 33% lower risk of cardiovascular mortality (p=0.06), and a 55% lower risk of infection-related mortality compared to HD. The incidence rates of dialysis sessions complicated by hypotension and of all-cause hospitalization were lower in patients assigned to online HDF. Results were consistent in distinct subgroups of patients according to age, sex, diabetes mellitus, the Charlson comorbidity index, and vascular access. The strengths of this study include the randomized design, the large sample size, and long follow-up, as well as the achievement of high convection volumes in vast majority of patients. This fact indicates that good clinical practices were performed in all facilities participating in this clinical trial (i.e., staff and care giver training, high blood flow, and relatively long dialysis time). Limitations of the study may include confounding factors such as imbalance in vascular access type, age, history of diabetes, Charlson Comorbidity Index, 6% low-flux treatments, transplantation rate and patient screening on blood flow performances (9,10). However, this was the first prospective, RCT showing that high-efficiency postdilution online HDF reduces all-cause mortality compared with high–flux HD, including in a post hoc re-analysis that included competing risk factors (11).
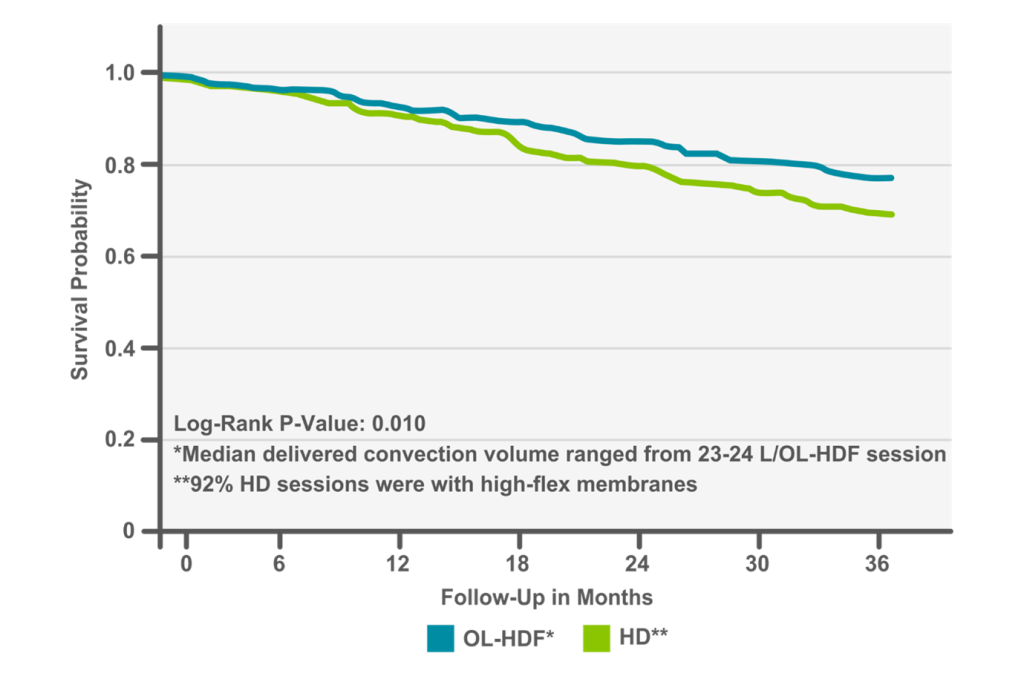 Figure 3. Increased overall survival in OL-HDF vs. HD (8) (p. 491).
Figure 3. Increased overall survival in OL-HDF vs. HD (8) (p. 491).
The fourth study was the French HDF study (FRENCHIE, French Convective HDF Study In Elderly). In the FRENCHIE study, a prospective, open-label randomized controlled trial, 381 elderly prevalent hemodialysis patients (over age 65) were randomly assigned in a one-to-one ratio to either high-flux HD or online postdilution HDF with 24 months follow-up (12). The median substitution volume achieved was 21 L/session overall for a targeted convection volume of 24 L/session. The primary outcome was intradialytic tolerance (day 30-day 120). The secondary outcome was a composite of all-cause and CV mortality, intermediary outcomes (i.e., biomarkers) and health-related quality of life. During the observational period for intradialytic tolerance, 85% and 84% of patients in high-flux hemodialysis and online hemodiafiltration arms, respectively, experienced at least one adverse event without significant difference between groups. In an exploratory analysis, intradialytic tolerance was also studied, using the sessions as a statistical unit according to treatment actually received. Over a total of 11,981 sessions, 2,935 were complicated by the occurrence of at least one adverse event, with a significantly lower occurrence in online hemodiafiltration with fewer episodes of intradialytic symptomatic hypotension and muscle cramps. More arrhythmia episodes were registered during the HDF sessions (p=0.01). In contrast, health-related quality of life, morbidity, and mortality were not different between groups. An improvement in the control of metabolic bone disease biomarkers and β2-microglobulin level, without change in serum albumin concentration, was observed with online hemodiafiltration (12). Although no significant difference in all-cause and cardiovascular mortality was observed between high-flux and HDF patients at 24 months, overall outcomes favored online hemodiafiltration over high-flux hemodialysis in the elderly (Figure 4). Notably, the study was underpowered and mortality in the ESKD population was low.
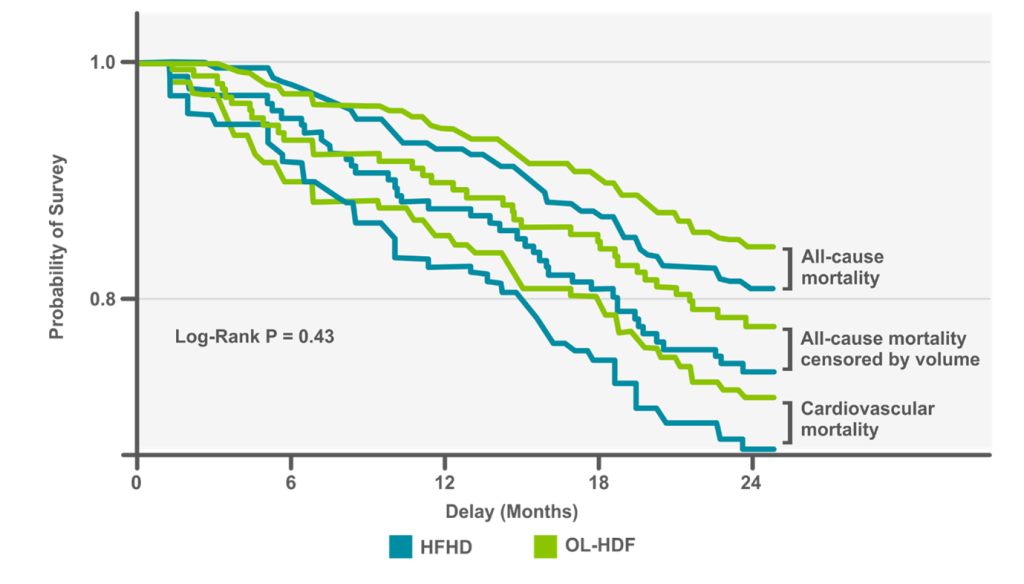 Figure 4. Increased overall survival in OL-HDF vs. HFHF in the elderly (12) (p. 1054).
Figure 4. Increased overall survival in OL-HDF vs. HFHF in the elderly (12) (p. 1054).
The fifth study was the CONVINCE trial, which was a pragmatic, open-label 1:1 randomized controlled trial that included 1360 adult HD patients from 61 dialysis centers across eight European countries (13). Six hundred and eighty-three patients were randomized to the high-volume HDF group and 677 were randomized to the high-flux HD group. All included patients in both groups were deemed to be candidates for achieving high convection volume targets (≥23 L/session). The primary outcome was all-cause mortality and secondary outcomes included sub-group analyses for cardiovascular, non-cardiovascular-, and infection-related-causes of death as well as fatal or non—fatal cardiovascular outcomes, kidney transplants, and hospitalizations. After a median follow-up of 30 months, the authors reported that the mean achieved convection volume in the HDF group was 25.2 liters per session and at least 23 ±1 liters of convection volume was achieved in 92% of delivered HDF treatments. The primary outcome of all-cause mortality was significantly lower in the HDF group compared to the high-flux HD group (HR=0.77; 95% CI: 0.65-0.93; p<0.05), equating to a 23% reduction in relative risk of all-cause mortality in the HDF group compared to the HD group. There were no significant differences between groups for cardiovascular (HR=0.81; 95% CI: 0.49-1.33) or non-COVID-19 infection-related deaths (HR=0.68; 95% CI: 0.42-1.10). Similarly, there were no significant differences in fatal or non-fatal cardiovascular outcomes (HR=1.07; 95% CI: 0.86-1.33), kidney transplants (HR=1.01; 95% CI: 0.71-1.44), or recurrent hospitalizations (for any non-fatal cause: HR=1.11, 95% CI: 0.98-1.25; infection-related including COVID-19: HR=1.06, 95% CI: 0.86-1.30; infection-related excluding COVID-19: HR=0.97, 95% CI: 0.74-1.26) between groups. There was an apparent reduction in non-cardiovascular deaths (HR= 0.76; 95% CI: 0.59-0.98) and infection-related deaths when including COVID-19 (HR=0.69; 95% CI: 0.49-0.96) however no adjustment for multiplicity was made and the 95% confidence intervals cannot be used in place of hypothesis testing for significance. Additionally, death from COVID-19 and death from cardiovascular causes could not be distinguished in patients with COVID-19 suggesting that these cause-specific results should be interpreted with caution. Notably, sub-group analyses showed no survival benefit for patients with a history of diabetes or cardiovascular disease at baseline while there was a benefit for those without a history of those two co-morbidities. Average blood flow rates (374 vs 369 mL/min) and Kt/V (1,74 vs 1.65) were higher in the HDF group compared to the HD group. This trial was limited due to lower sample size than anticipated (due to COVID-19), lower overall risk of death than expected, potential selection bias for patients with good vascular access and those able to complete outcome assessments.
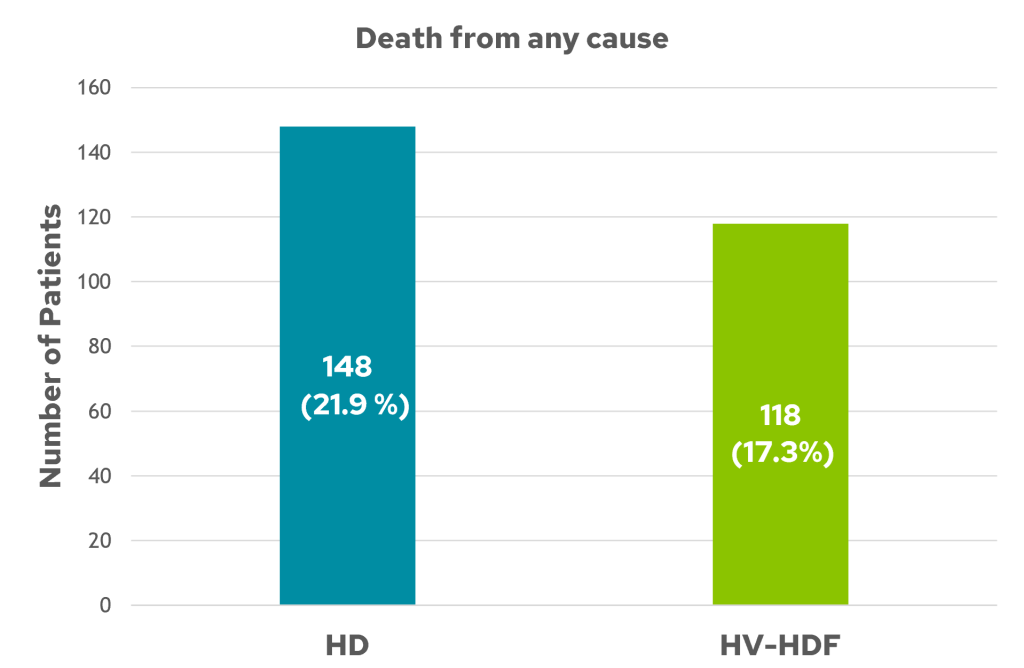 Figure 5. 23 % Lower rate of all-cause mortality in HDF vs. HD (13).
Figure 5. 23 % Lower rate of all-cause mortality in HDF vs. HD (13).
In brief, two prospective RCTs (CONTRAST and Turkish HDF studies) failed to show beneficial effects on all-cause or cardiovascular mortality in overall analyses. However, post hoc analyses of both studies showed beneficial effects in patients with high convection volumes (3,7). The ESHOL study, which achieved the highest median convection volume, demonstrated a 30% reduction in all-cause mortality in patients treated with high-volume HDF (8). The FRENCHIE study, which was performed in elderly patients, showed that HDF patients experienced significantly fewer episodes of symptomatic intradialytic hypotension and muscle cramps, while no differences were seen for health-related quality of life, morbidity, or mortality. Control of metabolic bone disease biomarkers and b2-microglobulin levels were much improved in the HDF group (12). The CONVINCE trial reported a 23% relative risk reduction in the HDF group (which achieved convection volumes of at least 23 ±1 liters in 92% of delivered HDF treatments) compared to high-flux HD, but no significant difference in cardiovascular mortality (13). A brief summary of the five RCT studies is presented in the Table 1.
Table 1. Overview of the CONTRAST (3), Turkish (7), ESHOL (8), FRENCHIE (12), and CONVINCE (13) postdilution HDF studies.
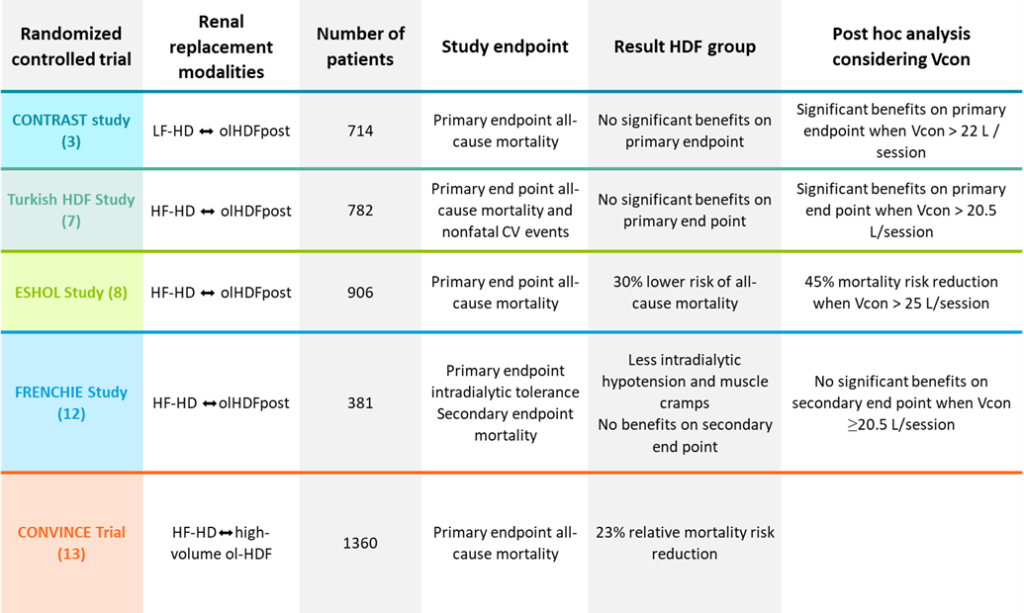
HF, High-Flux; LF, Low-Flux; HD, hemodialysis; HDF, hemodiafiltration: ol-HDF, online hemodiafiltration; Vcon convection volume, CV cardiovascular; CONTRAST Dutch Convective Transport Study; THDFS Turkish HDF Study; ESHOL Estudio de Super-vivencia de Hemodiafiltración On-Line; FRENCHIE French Convective HDF Study In Elderly.
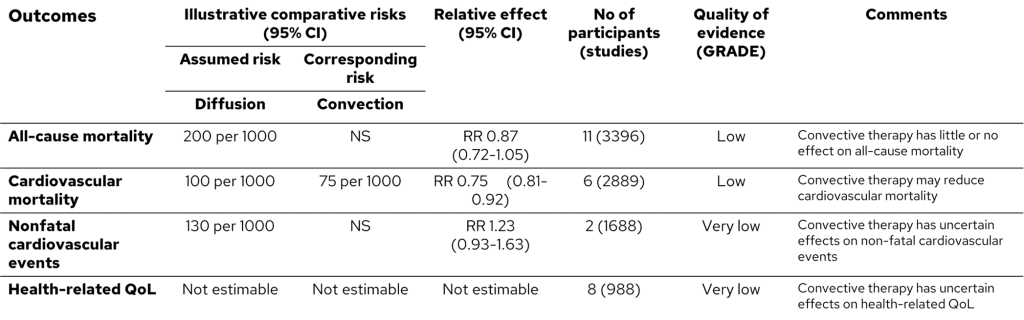
Historical meta-analyses and/or systematic reviews addressing benefits of HDF compared to standard HD have reported conflicting results (14-16). Unfortunately, some of these meta-analyses aggregated several different convection-based methods under the umbrella of “convective therapies” (i.e., hemofiltration, acetate-free biofiltration, low volume hemodiafiltration) and failure to account for the effective convection volume achieved presents a major shortcoming in their findings (17,18).
In their meta-analysis, Nistor et al. (15) compared mortality in patients on hemodiafiltration, hemofiltration, and acetate-free biofiltration to hemodialysis. Including low-convection volume treatments, such as offline hemofiltration/hemodiafiltration and acetate-free biofiltration, which can hardly be considered modern convective therapies, as the convection volumes of 10–12 L/session achieved are similar to the amount of internal filtration obtained with high-flux HD and different from high volume HDF (19,20). Another meta-analysis in which convection volume was included identified improved outcomes in patients receiving adequately dosed HDF (21). Therefore, data suggest that convective dialysis may reduce cardiovascular but not all-cause mortality, and that effects on nonfatal cardiovascular events and hospitalization are inconclusive, considering shortcomings in study methods and reporting (Table 2) (15).
Table 2. Mortality comparison of diffusive and convective therapies (15) (p. 3).
All reported studies (observational and interventional) support the notion that total convection volume delivered, regardless of substitution mode (i.e., post, pre, or mixed), on a regular basis matters. Convective dose represents the driving force for patient outcome improvement in a dose-dependent manner (22,23).
That a positive outcome depends on the convection volume was supported further by the results of analyses of individual-patient data meta-analysis (IPD-MA) from the CONTRAST study, ESHOL study, Turkish study, and FRENCHIE study (24). In aggregate, 2793 patients were included in these analyses. After a median follow-up of 2.5 years, 769 of the 2793 patients had died, with 292 of the deaths being cardiovascular. HDF patients were divided into tertiles based on delivered convection volume and all-cause and cardiovascular mortality were compared to that with HD (Figure 6). Hazard ratios were calculated using Cox proportional hazard regression models (24). In the first analysis, a survival benefit of online HDF was found for patients in the highest tertile of convection volume, but results varied depending on how convection volume was standardized to body size (25). All-cause mortality in the tertile receiving the highest convection volumes was reduced when the convection volume was not standardized, or standardized to body surface area or total body water (hazard ratios, 95% confidence intervals of 0.66 (0.52 – 0.83), 0.71 (0.57 – 0.90) and 0.71 (0.57 – 0.89), respectively). No reduction was found for standardization to body weight or body mass index. These results were confirmed in a second analysis where online HDF was shown to reduce all-cause mortality by 14% and cardiovascular mortality by 23% compared to HD. There was no evidence for a differential effect in pre-determined subgroups and, again, the largest survival benefit was for patients receiving the highest delivered convection volume (>23 L/1.73 m2 body surface area) (25). In a cause-specific analysis on mortality, it was also shown that HDF had a significant reduction effect on fatal cardiac events, including ischemic heart disease as well as congestion (26). It was then calculated that the patient number needed to treat by HDF in order to prevent one cardiovascular death was 75 per year.
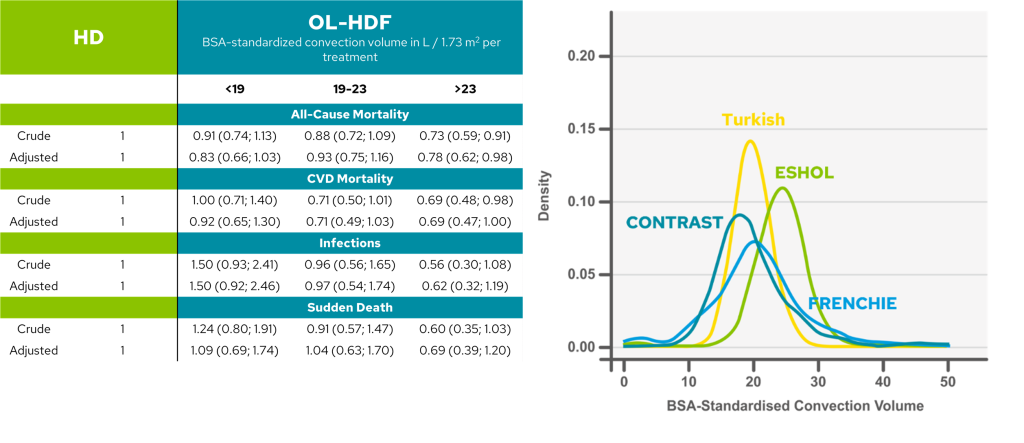 Figure 6. All-cause mortality decrease in tertile receiving highest, BSA-standardised convection volume (24) (p.981).
Figure 6. All-cause mortality decrease in tertile receiving highest, BSA-standardised convection volume (24) (p.981).
References:
- Canaud B, Bragg-Gresham JL, Marshall MR, Desmeules S, Gillespie BW, Depner T, et al. Mortality risk for patients receiving hemodiafiltration versus hemodialysis: European results from the DOPPS. Kidney Int. 2006;69(11):2087-93.
- Penne EL, Blankestijn PJ, Bots ML, van den Dorpel MA, Grooteman MP, Nubé MJ, et al. Effect of increased convective clearance by on-line hemodiafiltration on all cause and cardiovascular mortality in chronic hemodialysis patients – the Dutch CONvective TRAnsport STudy (CONTRAST): rationale and design of a randomised controlled trial [ISRCTN38365125]. Curr Control Trials Cardiovasc Med. 2005;6(1):8.
- Grooteman MP, van den Dorpel MA, Bots ML, Penne EL, van der Weerd NC, Mazairac AH, et al. Effect of online hemodiafiltration on all-cause mortality and cardiovascular outcomes. J Am Soc Nephrol. 2012;23(6):1087-96.
- Chapdelaine I, de Roij van Zuijdewijn CL, Mostovaya IM, Lévesque R, Davenport A, Blankestijn PJ, et al. Optimization of the convection volume in online post-dilution haemodiafiltration: practical and technical issues. Clin Kidney J. 2015;8(2):191-8.
- Chapdelaine I, Mostovaya IM, Blankestijn PJ, Bots ML, van den Dorpel MA, Levesque R, et al. Treatment policy rather than patient characteristics determines convection volume in online post-dilution hemodiafiltration. Blood Purif. 2014;37(3):229-37.
- de Roij van Zuijdewijn CLM, Chapdelaine I, Nubé MJ, Blankestijn PJ, Bots ML, Konings C, et al. Achieving high convection volumes in postdilution online hemodiafiltration: a prospective multicenter study. Clin Kidney J. 2017;10(6):804-12.
- Ok E, Asci G, Toz H, Ok ES, Kircelli F, Yilmaz M, et al. Mortality and cardiovascular events in online haemodiafiltration (OL-HDF) compared with high-flux dialysis: results from the Turkish OL-HDF Study. Nephrol Dial Transplant. 2013;28(1):192-202.
- Maduell F, Moreso F, Pons M, Ramos R, Mora-Macià J, Carreras J, et al. High-efficiency postdilution online hemodiafiltration reduces all-cause mortality in hemodialysis patients. J Am Soc Nephrol. 2013;24(3):487-97.
- Mann JF. How does hemodiafiltration improve survival? Kidney Int. 2013;84(6):1287-8.
- Farrington K, Davenport A. The ESHOL study: hemodiafiltration improves survival-but how? Kidney Int. 2013;83(6):979-81.
- Maduell F, Moreso F, Mora-Macià J, Pons M, Ramos R, Carreras J, et al. ESHOL study reanalysis: All-cause mortality considered by competing risks and time-dependent covariates for renal transplantation. 2016;36(2):156-63.
- Morena M, Jaussent A, Chalabi L, Leray-Moragues H, Chenine L, Debure A, et al. Treatment tolerance and patient-reported outcomes favor online hemodiafiltration compared to high-flux hemodialysis in the elderly. Kidney Int. 2017;91(6):1495-509.
- Blankestijn PJ, Vernooij RWM, Hockham C, et al. Effect of Hemodiafiltration or Hemodialysis on Mortality in Kidney Failure. N Engl J Med. 2023;389(8):700-709.
- Nistor I, Palmer SC, Craig JC, Saglimbene V, Vecchio M, Covic A, et al. Convective versus diffusive dialysis therapies for chronic kidney failure: an updated systematic review of randomized controlled trials. Am J Kidney Dis. 2014;63(6):954-67.
- Nistor I, Palmer SC, Craig JC, Saglimbene V, Vecchio M, Covic A, et al. Haemodiafiltration, haemofiltration and haemodialysis for end-stage kidney disease. Cochrane Database Syst Rev. 2015(5):Cd006258.
- Wang AY, Ninomiya T, Al-Kahwa A, Perkovic V, Gallagher MP, Hawley C, et al. Effect of hemodiafiltration or hemofiltration compared with hemodialysis on mortality and cardiovascular disease in chronic kidney failure: a systematic review and meta-analysis of randomized trials. Am J Kidney Dis. 2014;63(6):968-78.
- Susantitaphong P, Siribamrungwong M, Jaber BL. Convective therapies versus low-flux hemodialysis for chronic kidney failure: a meta-analysis of randomized controlled trials. Nephrol Dial Transplant. 2013;28(11):2859-74
- Rabindranath KS, Strippoli GF, Roderick P, Wallace SA, MacLeod AM, Daly C. Comparison of hemodialysis, hemofiltration, and acetate-free biofiltration for ESRD: systematic review. Am J Kidney Dis. 2005;45(3):437-47.
- Grooteman MP, Nubé MJ, Bots ML. Clinical Trials on Hemodiafiltration. Springer International Publishing Switzerland 2016 Nubé MJ et al. (eds.), Hemodiafiltration: Theory, Technology and Clinical Practice. ISBN 978-3-319-23331-4
- Basile C, Davenport A, Blankestijn PJ. Why choose high volume online post-dilution hemodiafiltration? J Nephrol 2017; 30:181–186
- Mostovaya IM, Blankestijn PJ, Bots ML, Covic A, Davenport A, Grooteman MP, et al. Clinical evidence on hemodiafiltration: a systematic review and a meta-analysis. Semin Dial. 2014;27(2):119-27.
- Maduell F. Is There an ‘Optimal Dose’ of Hemodiafiltration? Blood Purif. 2015;40 Suppl 1:17-23.
- Canaud B, Koehler K, Bowry S, Stuard S. What Is the Optimal Target Convective Volume in On-Line Hemodiafiltration Therapy? Contrib Nephrol. 2017;189:9-16.
- Peters SA, Bots ML, Canaud B, Davenport A, Grooteman MP, Kircelli F, et al. Haemodiafiltration and mortality in end-stage kidney disease patients: a pooled individual participant data analysis from four randomized controlled trials. Nephrol Dial Transplant. 2016;31(6):978-84.
- Davenport A, Peters SA, Bots ML, Canaud B, Grooteman MP, Asci G, et al. Higher convection volume exchange with online hemodiafiltration is associated with survival advantage for dialysis patients: the effect of adjustment for body size. Kidney Int. 2016;89(1):193-9.
- Nubé MJ, Peters SAE, Blankestijn PJ, Canaud B, Davenport A, Grooteman MPC, et al. Mortality reduction by post-dilution online-haemodiafiltration: a cause-specific analysis. Nephrol Dial Transplant. 2017;32(3):548-55.
*The CONVINCE study was exclusively supported by the European Commission Research & Innovation, Horizon 2020, Call H2020-SC1-2016-2017 under the topic SC1-PM-10-2017: Comparing the effectiveness of existing healthcare interventions in the adult population (grant no 754803). Disclaimer: The information in this document is provided as is and no guarantee or warranty is given that the information is fit for any particular purpose. The user thereof uses the information at its sole risk and liability.
The opinions expressed in the document are of the authors only and in no way reflect the European Commission’s opinions.

GMO-001149 Rev B 06/2024