
Factors Affecting Convection Volume in Online Hemodiafiltration (OL-HDF)
Several factors affect the achievement of convection volume during hemodiafiltration (HDF). The first are patient characteristics, such as vascular access type, vascular access flow, total protein level, and hematocrit. The second are modifiable factors associated with the dialysis prescription and best nursing care practices, such as the dialyzer type, the selected arterial and venous needles, level of blood flow rate (within the limit allowed by the vascular access), filtration fraction, and the duration of the dialysis session.
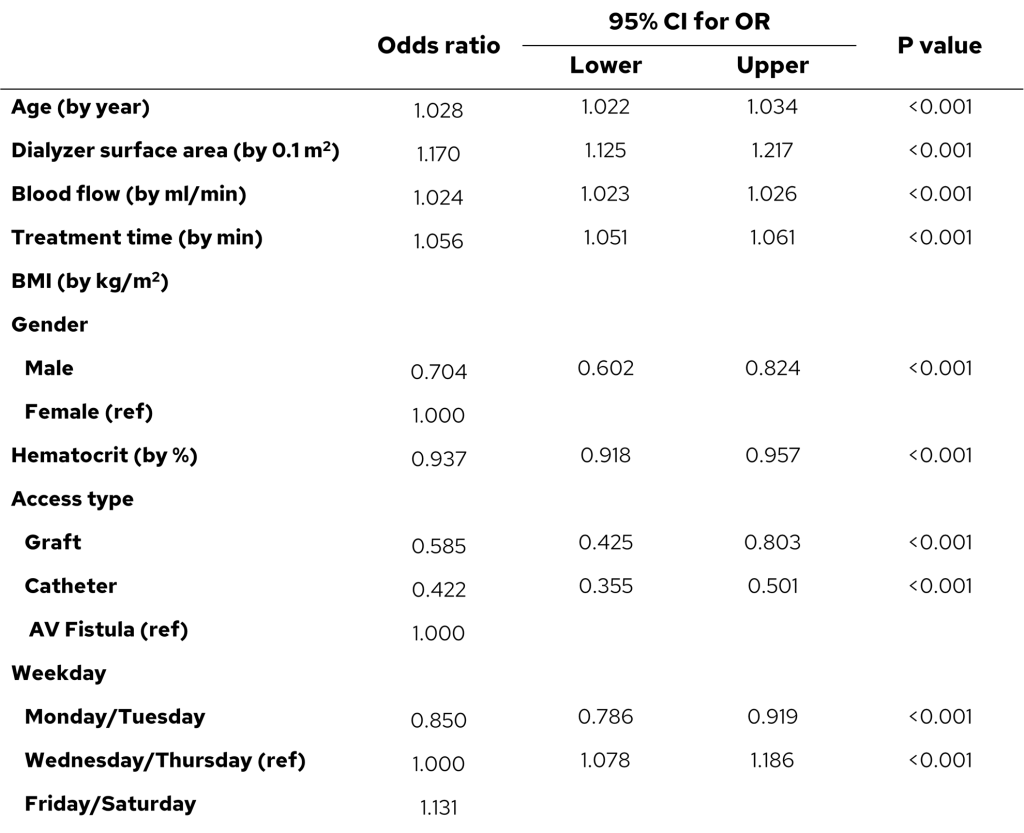
Marcelli D et al.1 investigated factors associated with the successful achievement of ≥21 L/session of substitution fluid volume in 3315 patients treated in six European countries on post-dilution hemodiafiltration. Mean blood flow was 379 ± 68 mL/min. Median substitution volume was 24.7 L (IQR 22.0–27.4 L). Mean filtration fraction was 28.3 ± 4.1%. The majority of sessions (81.5%) qualified as high-volume HDF (i.e., substitution volumes ≥21 L). Older age, and higher dialyzer surface area, blood flow, and treatment time were positively associated with the achievement of ≥21 L substitution volume; higher body mass index, male gender, higher hematocrit, graft or catheter vs. fistula, and start of week vs. mid-week were negatively associated, as shown in Table 1.
Table 1. Factors associated with the achievement of ≥21 L/session of substitution fluid.
Additionally, Chapdelaine I et al. demonstrated that treatment time and blood flow rate were major determinants of convection volume (Table 2). The magnitude of convection volume has typically relied on center policy rather than individualized patient prescription 2, using filtration fractions of at least 20%. Penne E et al. evaluated potential patient- and treatment-related determinants of convective volume in 235 patients on post-dilution HDF using multivariable linear regression models 3. The authors concluded that, in addition to treatment time and blood flow rate, convective volumes may be optimized by increasing the filtration fraction.
Table 2. Determinants of convection volume: uni- and multivariable linear regression analyses.

B-change of total convection volume (L/treatment) related with 1 unit increment of the determinant; Std B-change of total convection volume when the independent variable changes by 1 SD; R2 of multivariable model is 0.59.
One study prospectively investigated the feasibility of achieving and maintaining high convection volumes with online post dilution OL-HDF (high-volume HDF, defined as ≥22 L convection volume/session) in clinical practice, regardless of preexisting patient profiles. In a stepwise fashion, treatment time, blood flow rate and filtration fraction were optimized. After the optimization phase, 71/86 participants (83%) reached a convection volume of ≥22 L/session (mean 25.5 ± 3.6). At Week 4, 64/86 participants (74%) reached a convection volume of ≥22 L/session, and 66/83 (80%) at Week 8 mean convection volumes of 26.2 ± 3.6 and 26.0 ± 3.4 L/session, respectively (Figure 1). Of 4176 sessions, 79% were classified as high-volume HDF (≥21 L substitution volume/session, corresponding to 23.4 L convection volume/session). The patients achieved high convection volume irrespective of age, body size, or comorbidities. Only incremental adjustments in blood flow rate and filtration fraction alone were sufficient to obtain the high convection volume4. Importantly, the high convection volumes were not associated with undesirable pressure changes. However, the study is limited due to selection bias and the blood flow was not independently checked.
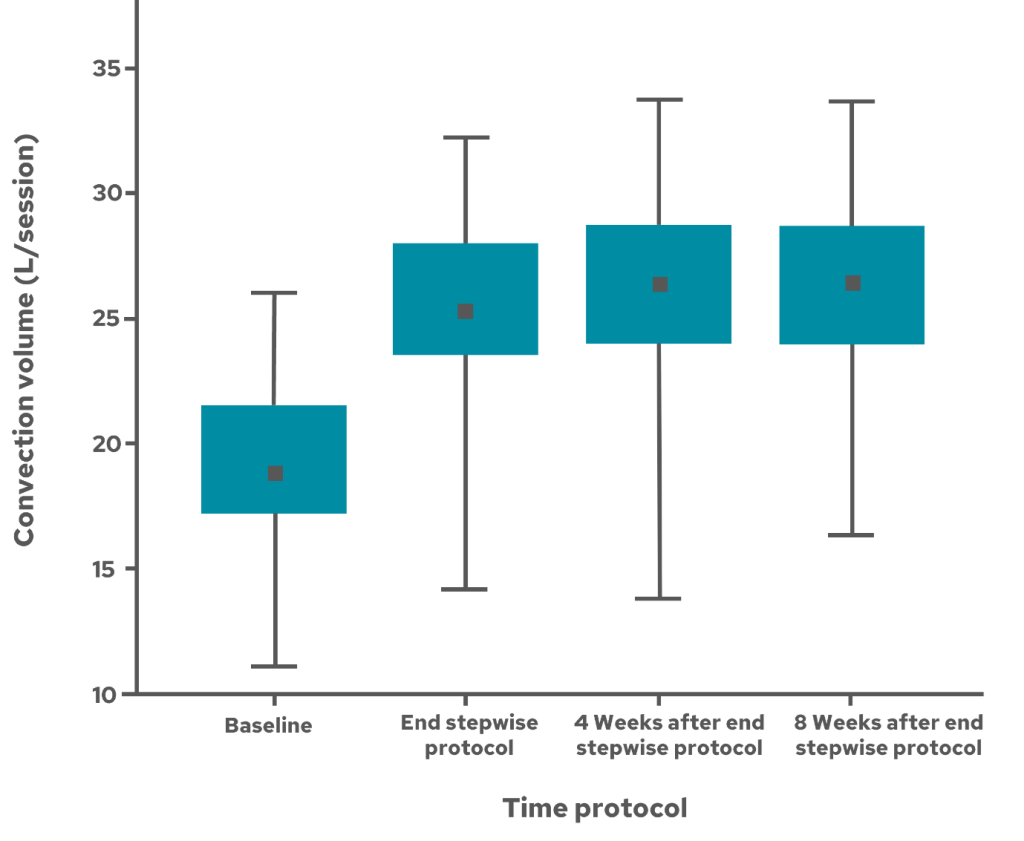
Figure 1. Stepwise optimisation of treatment time, blood flow rate, and filtration fraction in achieving high-volume OL-HDF.
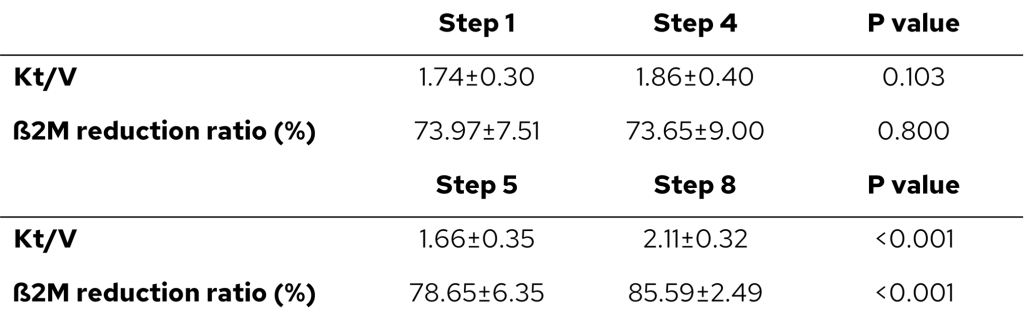
Another prospective study aimed to optimize methods for achieving a high convection volume in patients undergoing online HDF. One study investigated 30 patients undergoing hemodialysis, where a stepwise protocol was implemented by gradually increasing the blood flow rate (BFR; 280 to 300 to 330 ml/min in steps 1-3 and again on steps 5-7) and needle size (16 to 15 G; in step 4). The dialyzer with a surface area of 1.8 m2 was used in steps 1-4 and dialyzer with a surface area of 2.5 m2 was used in steps 5-8. The mean substitution volume was 18.7 ± 2.2 L at step 1, significantly increasing to 25.1 ± 2.6 L by step 8. A substitution volume of 21 L was achieved by 13.3% of patients in step 1 and by 96.7% after step 8. The substitution volume was higher for the dialyzer with a large surface area and for the larger needle size used (15 G). Between steps 5 and 8, the Kt/V and β2 microglobulin reduction ratio improved significantly. The changes in spkt/v and β2 microglobulin reduction ratio were not significant from steps 1-4 (Table 3).
Table 3. Increase of Kt/V and ß2M RR in higher convection volumes.
The study demonstrated that an increase in the convection volume can be obtained independent of the patient’s clinical characteristics, through a structured, stepwise protocol with an incremental adjustment of BFR, needle size and using a dialyzer with a large surface area5. However, the study is limited due to small sample size and using only two kinds of dialyzer and needle size, hence generalizability to real-world setting may be low.
References:
- Marcelli D, Kopperschmidt P, Bayh I, et al. Modifiable factors associated with achievement of high-volume post-dilution hemodiafiltration: results from an international study. Int J Artif Organs. 2015;38(5):244-250. Available from: http://www.ncbi.nlm.nih.gov/pubmed/26080930.
- Chapdelaine I, Mostovaya IM, Blankestijn PJ, et al. Treatment Policy rather than Patient Characteristics Determines Convection Volume in Online Post-Dilution Hemodiafiltration. Blood Purif. 2014;37(3):229-237. Available from: http://www.ncbi.nlm.nih.gov/pubmed/24943743.
- Penne EL, van der Weerd NC, Bots ML, et al. Patient- and treatment-related determinants of convective volume in post-dilution haemodiafiltration in clinical practice. Nephrol Dial Transplant. 2009;24(11):3493-3499. Available from: http://www.ncbi.nlm.nih.gov/pubmed/19515802.
- de Roij van Zuijdewijn CLM, Chapdelaine I, Nubé MJ, et al. Achieving high convection volumes in postdilution online hemodiafiltration: a prospective multicenter study. Clin Kidney J. 2017;10(6):804-812. Available from: https://www.ncbi.nlm.nih.gov/pubmed/29225810.
- Kim DH, Lee Y-K, Park HC, et al. Stepwise achievement of high convection volume in post-dilution hemodiafiltration: A prospective observational study. Semin Dial. Published online March 2021.
GMO-000123 Rev B 05/2024