
Continuous Kidney Replacement Therapy (CKRT)
Introduction:
Continuous Kidney Replacement Therapy (CKRT), formerly known as Continuous Renal Replacement Therapy (CRRT), is an extracorporeal clearance modality intended to replace the solute and fluid homeostasis functions of the kidneys in patients with renal failure (1). CKRT was first introduced in 1977 with the use of continuous arteriovenous hemofiltration (CAVH) in Germany, using both the heart and arterial pressure as the pumping mechanism (2). Over the past four decades, the advancement of CKRT technologies has led to the advent of continuous veno-venous hemofiltration (CVVH), continuous veno-venous hemodialysis (CVVHD), and continuous veno-venous hemodiafiltration (CVVHDF). Each of the three modalities can be differentiated by mechanisms of fluid management, solute transport, and use of substitution and dialysate fluid (1).
Population:
CKRT is most commonly used in patients with acute illness, and more specifically those with persistent or progressive acute kidney injury (AKI) with hemodynamic instability or risk of increased intracranial pressure (ICP). Some intensive care unit (ICU) patients can be managed with intermittent hemodialysis (IHD);, however, 5% to 10% of ICU patients being treated for AKI will require kidney replacement therapy (KRT)RRT. Those that require RRT KRT have a mortality rate of 30% to 70%; thus, selection of the proper administration techniques and indications of CKRT are necessary (3,4).
Indications:
Disease states in which CKRT may be indicated include AKI, metabolic acidosis, electrolyte abnormalities (i.e., hyperkalemia, hyponatremia, and hyperphosphatemia), anemia, uremia, heart failure, acute brain injury, sepsis and multiorgan failure, and removal of toxic substances or poisons (1).
Components Needed for Performing CKRT:
When performing CKRT, there are several key components that are necessary for this modality. The CKRT machine itself is necessary, as well as a dialyzer, vascular access site, dialysate and the respective administration rate and components, dose of anticoagulant, duration of therapy, and the CKRT prescription (4).
Dialyzer:
The dialyzer functions to remove both solute and solvent and is often referred to as an artificial kidney. The dialyzer, or filter, types also help determine which solutes may be removed during CKRT. For example, super-high-flux dialyzers are useful for preventing rhabdomyolysis-induced AKI due to their ability to remove myoglobin (1). Dialyzers in CKRT are mostly made of hollow synthetic fibers rather than cellulosic membranes. Synthetic membranes are favored over the historic cellulosic membranes since they can absorb plasma proteins, forming what is known as a secondary membrane and can further direct water permeability (4).
Vascular Access:
Proper functioning of the vascular access points is critical in CKRT since inadequate access function such as flow, obstruction, and narrowing, may result in insufficient blood flow and thus an overall decreased efficacy of the dialysis treatment. Kidney Disease Improving Global Outcomes (KDIGO) guidelines recommend the following order for venous access placement: right internal jugular vein, femoral vein as a second line option for obese patients due to higher risks of malfunction and mortality, left internal jugular vein, subclavian vein on the dominant side, then subclavian vein on the non-dominant side used only as a rescue option (1,4,6). The right internal jugular vein is preferred for catheter placement since it allows for direct access to the superior vena cava. Currently, temporary or cuffed hemodialysis catheters may be used in CKRT following placement via ultrasound. The reasoning behind the use of tunneled or cuffed catheters is the ability to achieve higher Qb due to their large diameters (1). According to the KDIGO guidelines, various catheter lengths should be used at the different access sites. An internal jugular vein catheter should be 12-15 cm, while a catheter at the femoral vein should be 19-24 cm and placed 15-20 cm left of the internal jugular vein (5). Proper catheter positioning is also crucial for adequate functioning and relies heavily on catheter size (3).
Substitution Fluid:
Substitution fluids, which are used to replenish electrolytes and fluid volume, are made up of both electrolytes and buffers to correct metabolic abnormalities (1). Hypernatremia, hyponatremia, hyperkalemia, and hypomagnesemia are all common electrolyte abnormalities that can be corrected by altering the substitution fluid. Buffer solutions include lactate or bicarbonate solutions. KDIGO guidelines recommend the use of bicarbonate buffers over lactate (5). Substitution fluids may be introduced before the dialyzer, or pre-dilution, or after the dialyzer, described as post-dilution. The use of pre-dilution substitution fluid decreases the risk of clotting at the filter and dilutes the concentration gradient between the blood and dialysate, which can decrease clearance of solute. Conversely, post-dilution substitution fluid may increase the risk of clotting at the filter; however, it also increases the clearance of solutes during CKRT due to an increased concentration gradient across the dialyzer membrane. Substitution fluid rates (Qs) should be maintained between 1,000 to 2,000 mL/hr to maintain fluid balance (1).
Initiation and Duration of therapy:
A controversial topic facing CKRT is the timing of both initiation and termination of therapy (4). There are no definitive guidelines and prevailing recommendations are based on broad definitions. For instance, according to KDIGO guidelines, CKRT should be initiated emergently when abnormalities in fluid, electrolytes, or acid-base balance are life-threatening to the patient and should be assessed based on trends in laboratory testing rather than a stand-alone, single lab (4,6).
CKRT Prescription:
The CKRT prescription is expressed as effluent dose, or the volume of blood purified per kilogram per hour, with a goal of 20-25 mL/kg/hr. In fact, studies show that doses greater than 25 mL/kg/hr do not significantly decrease mortality in patients with AKI while doses greater than 50 mL/kg/hr increase the rates of hypophosphatemia and hypokalemia among this patient population. A 2009 multicenter randomized control trial comparing high dose effluent rate (40 mL/kg/hr) (n=747) versus low dose effluent rate (25 mL/kg/hr) (n=761) in CKRT for patients experiencing AKI showed lower or similar mortality rates across groups at 90 days post randomization (p=0.99). Hypophosphatemia was more common in the high intensity group compared to the lower intensity group (p<0.001). At 90 days post randomization, less patients in the lower intensity group were still receiving therapy at 4.4% versus 6.8%, respectively, though this was not statistically significant (p=0.14) (6). Effluent volume rate can be calculated based on Equation 1 below (7).

Filtration Fraction:
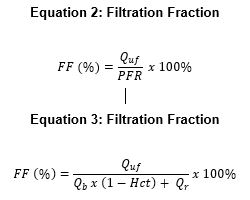
Filtration Fraction (FF) is described as the ratio of the net rate of plasma water removal or ultrafiltration rate (Quf) to the plasma flow rate (PFR) at the filter. Of note, the PFR is equal to the blood flow rate (BFR, Qb) multiplied by 1 minus the measured hematocrit level (Hct) plus the replacement rate ( ). FF may be calculated using Equation 2 or Equation 3 when pre-dilution replacement fluid is used. The FF goal in CKRT should be < 25 in order to minimize poor filter performance and clotting (1).
Solute Removal Techniques:
CKRT modalities are differentiated according to the mechanism by which clearance occurs. The four main mechanisms involved in solute clearance are diffusion, convection, ultrafiltration, or a combination of both convection and diffusion.
Diffusion:
Diffusion is defined as the movement of solutes from a region of higher concentration gradient to one of lower concentration gradient, with the eventual establishing of an equilibrium between the solutes. In hemodialysis, a solute gradient is established between the blood and the dialysate across the dialyzer membrane. Smaller molecule weight molecules tend to move across the membrane faster than larger ones (3).
Convection:
Convection is the process of solute removal across a membrane due to solvent drag, also called solvent drag (8). The main limitation to convection is the size of the pores within the hemofilter itself. Clearance of solutes of both low and high molecular weights are similar until the solute size is about equal to the filter pore size (3).
Osmosis/Ultrafiltration:
Ultrafiltration can be defined as the movement of water across a semi-permeable membrane due to a pressure gradient. The blood flow from the patient entering into the dialyzer has a higher pressure than the transmembrane pressure, thus water, and solutes, move from the high pressure environment to the lower pressure environment (3). The ultrafiltration rate (Quf) can vary between the different CKRT modalities.
CKRT Modalities:
CKRT more closely mimics the normal kidney function compared to intermittent hemodialysis (IHD) and consists of four main modalities, including CVVHD (Figure 3), CVVH (Figure 4), CVVHDF (Figure 5), and SCUF (Figure 6) (9). Clinician preference as well as method specific solute removal both play a role in the choice of CKRT modality. The Qb of all CKRT modalities are similar and between 100 to 350 mL/min with the exception of SCUF that suggest a Qb between 100 to 200 mL/min (1). The differences in mechanism of solute removal between these modalities is discussed below in Figure 1.
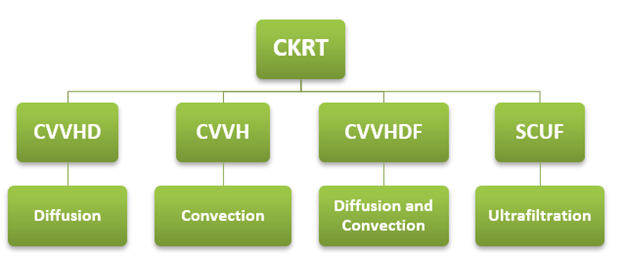
Figure 1: Types of CKRT Modalities and solute clearance mechanisms.
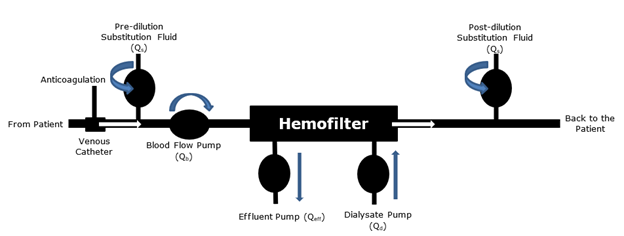
Figure 2: Simplistic CKRT circuit set up.
CVVHD:
CVVHD provides both solute clearance as well as volume removal. It consists primarily of diffusive clearance where the membrane gradient is established by both the dialysis fluid flow rate (Qd) and the Qb. CVVHD is extremely effective for removing solutes with lower molecular weights such as potassium, urea, and creatinine. Ultrafiltration rates are slower in CVVHD than CVVH (3). Studies suggest that the dialysate flow rate (Qd) in CVVHD should be between 1,000 to 2,000 mL/hr while the Quf should be between 2 to 8 mL/min. The Qeff should be between 24 to 48 L/day (1). It does not require substitution fluid.
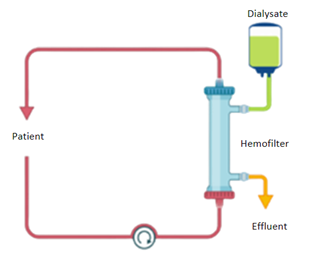
Figure 3: Schematic of CVVHD circuit.
CVVH:
CVVH is a convection-based CKRT that consists of an ultrafiltrate passing through a transmembrane pressure (TMP) gradient in order to achieve solute removal. CVVH requires substitution fluid that may be delivered either pre- or post-dilution (1). Since CVVH works via a convection mechanism, solutes are removed at a higher clearance in comparison to CVVHD (3). Additionally, some clinicians prefer CVVH because pure convection can remove a larger number of molecules than diffusive based therapies (8). The Quf CVVH should be between 16 to 33 mL/min with a Qeff between 24 to 48 L/day (1).
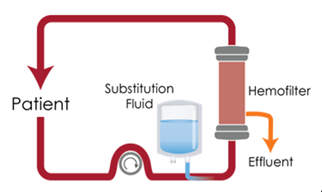
Figure 4: Schematic of CVVH circuit shown with pre-dilution substitution fluid.
CVVHDF:
CVVHDF is the combination of both CVVH and CVVHD, removing solutes by both convection and diffusion. It should maintain a Qd of 1,000 to 2,000 mL/hr (1). The Qeff for CVVHDF should be between 48 to 96 L/day (1).
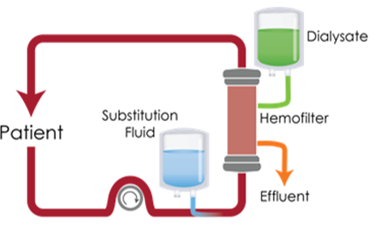
Figure 5: Schematic of CVVHDF circuit shown with post-dilution substitution fluid.
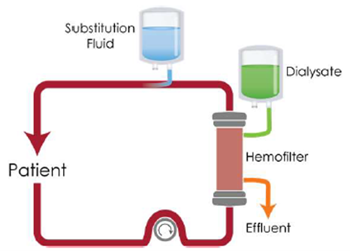
Figure 6: Schematic of CVVHDF circuit shown with pre-dilution substitution fluid.
SCUF:
In SCUF, water is removed via ultrafiltration and is useful for patients experiencing fluid overload that do not require solute removal. Qeff for SCUF should be between 2 to 8 L/day (1).
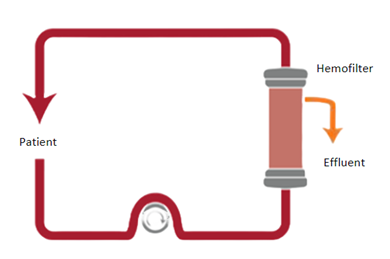
Figure 7: Schematic of SCUF circuit.
Advantages and Disadvantages of CKRT:
Advantages:
One advantage of CKRT over other dialysis modalities is the continuous removal of toxins and fluid, thus mimicking natural kidney function. Furthermore, CKRT provides a benefit to overall hemodynamic stability, fluid balance, and a minimizes the overall risk of increased intracranial pressure (5).
Disadvantages:
Due to the continuous nature of CKRT, solutes or toxins are removed at a slower clearance rate than other dialysis modalities. Additionally, CKRT often requires the use of anticoagulants due to the increased risk of thrombosis. Since CKRT is a 24-hour blood purification method, patient mobility is substantially limited. Other disadvantages that one must take into consideration is the risk of hypothermia and increased costs of CKRT therapy (5).
Complications:
Though CKRT provides an effective option for blood purification, it does not come without consequences. Common complications of CKRT are similar to those experienced in intermittent hemodialysis and include vascular access complications, infections, fluid imbalances, thrombosis, and lactic acidosis.
Vascular Access Complications:
Catheter-related complications include hemorrhaging, infections, venous thrombosis and stenosis, pneumothorax, hemothorax, air embolism, and visceral injury (3). The use of ultrasound visualization techniques helps to ensure safe and proper catheter placement. Finally, it is recommended to keep the catheter in view to avoid accidental disconnections that may cause severe blood loss (10).
Infections:
Though they are not routinely recommended, tunneled catheters are known to cause decreased rates of infections. However, they may provide benefits in patients requiring CKRT for greater than one to three weeks (3). Furthermore, the use of antibiotic covered catheters may provide additional benefit against bacterial infections (10). Studies suggest that evaluation of changed to the volume of distribution (Vd) and plasma protein levels as wells as nonrenal clearance and residual renal function if antibiotics or other drug therapies are added to the regimen to avoid supratherapeutic or subtherapeutic concentrations (3).
Fluid & Electrolyte Imbalances:
CKRT can lead to electrolyte abnormalities such as hypophosphatemia, hypokalemia, hypocalcemia, and hypomagnesemia. Improper dialysate electrolyte concentrations may also lead to hyponatremia, hypernatremia, or hyperkalemia. Electrolyte imbalances are common in CKRT patients and thus should be monitored daily during CKRT therapy (3).
Hypothermia:
Hypothermia is a common complication of CKRT since large volumes of the patient’s blood circulate in the extracorporeal circuit throughout therapy, as well as the lack of dialysate and substitution fluids being warmed (1). In fact, hypothermia is seen in about one-third of CKRT patients. Hypothermia leads to vasoconstriction and can thus increase the risk of hemodynamic instability (3). Hypothermia may also mask the presence of fevers and thus making infections more difficult to diagnose and antibiotic therapy delayed in patients experiencing hypothermia. Warming blankets are useful to help combat hypothermia (10).
Anticoagulation and Thrombosis:
The 2012 KDIGO guidelines recommend the use of regional citrate for anticoagulation in CKRT rather than systemic heparin in patients without contraindication. Of note, citrate is currently used off-label for anti-thrombotic effects in CKRT therapy and is not approved by the FDA for use with any CKRT device. When a contraindication to citrate is present, either unfractionated heparin (UFH) or low molecular weight heparin (LMWH) are the anticoagulants of choice. Additionally, KDIGO guidelines recommend that for patients with an increased risk of bleeding, regional citrate is also preferred. For those with contraindications to citrate and an increased bleed risk, KDIGO advises against the use of regional heparin and states that CKRT should be administered without anticoagulation (5). It is important to be aware of the possibility of the development of metabolic alkalosis when using citrate due to the metabolism of citrate to bicarbonate in a 1:3 ratio. On the contrary, citrate may lead to lactic acidosis in those with impaired liver function due to citrate accumulation and increased anion-gaps (3). Of note, heparin exerts its anticoagulatory effects by binding thrombin and factor Xa and is monitored by APTT. However, heparin has the ability to bind to other positively charged proteins which is a main limitation of its use due to variability of its response (11).
In summary, CKRT is an extracorporeal clearance modality intended to replace the solute and fluid homeostasis functions of the kidneys in patients with renal failure. CKRT utilizes diffusion, convection, and ultrafiltration to remove fluid and solutes from the blood. When initiating CKRT, it is important to have all of the necessary components, including the CKRT machine, dialyzer, vascular access site, dialysate and the respective administration rate and components, dose of anticoagulant, duration of therapy, and the CKRT prescription. The four modalities that may be utilized in CKRT are CVVHD, CVVH, CVVHDF, and SCUF. There are a number of advantages and disadvantages associated with each modality, and the decision to initiate one over another should be made by the physician after careful evaluation of the individual patient.
References:
-
- Macedo E, Mehta RL. Continuous Dialysis Therapies: Core Curriculum 2016. Am J Kidney Dis. 2016;68(4):645-657.
- Ronco C, Bellomo R, Kellum JA. Continuous renal replacement therapy: Opinions and evidence. Adv Ren Replace Ther. 2002;9(4):229-244. www.ncbi.nlm.nih.gov/pubmed/12382223
- Karkar A, Ronco C. Prescription of CRRT: a pathway to optimize therapy. Ann Intensive Care. 2020;10(1). www.ncbi.nlm.nih.gov/pubmed/32144519
- Clark WR, Gao D, Lorenzin A, Ronco C. Membranes and Sorbents. Contrib Nephrol. 2018;194:70-79. www.ncbi.nlm.nih.gov/pubmed/29597218
- KDIGO. KDIGO clinical practice guideline for acute kidney injury. Kidney Int Suppl. 2012;2(1):89-115.
- Palevsky PM, Zhang JH, O’Connor TZ, Chertow GM, Crowley ST, Choudhury D, Finkel K, Kellum JA, Paganini E, Schein RMH, Smith MW, Swanson KM, Thompson BT, Vijayan A, Watnick S, Star RA, Peduzzi P. Intensity of renal support in critically ill patients with acute kidney injury. N Engl J Med. 2008;359(1):7-20. www.ncbi.nlm.nih.gov/pubmed/18492867
- Claure-Del Granado R, Macedo E, Chertow GM, Soroko S, Himmelfarb J, Ikizler TA, Paganini EP, Mehta RL. Effluent volume in continuous renal replacement therapy overestimates the delivered dose of dialysis. Clin J Am Soc Nephrol. 2011;6(3):467-475.
- Cerdá J, Ronco C. Modalities of continuous renal replacement therapy: technical and clinical considerations. Semin Dial. 22(2):114-22. www.ncbi.nlm.nih.gov/pubmed/19426413
- Tandukar S, Palevsky PM. Continuous Renal Replacement Therapy: Who, When, Why, and How. Chest. 2019;155(3):626-638. www.ncbi.nlm.nih.gov/pubmed/30266628
- Finkel KW, Podoll AS. Complications of continuous renal replacement therapy. Semin Dial. 2009;22(2):155-159.
- Hirsh J, Anand SS, Halperin JL, Fuster V. Mechanism of action and pharmacology of unfractionated heparin. Arterioscler Thromb Vasc Biol. 2001;21(7):1094-1096. www.ncbi.nlm.nih.gov/pubmed/11451734
GMO-000410 Rev A 03/2024