
Chapter 2 | From Conventional Hemodialysis to High-Volume Hemodiafiltration
2.1 | Introduction
The profile of patients transitioning from chronic kidney disease (CKD) to maintenance hemodialysis (HD) is shifting toward an older population with multiple comorbid conditions (notably diabetes mellitus and heart failure). Despite improvements in dialysis care, overall survival for ESKD patients on HD remains poor. Cardiovascular disease is the single largest cause of mortality in this population; according to the 2023 United States Renal Data System Annual Data Report, over half (52.2%) of deaths with a known cause were related to cardiovascular disease (47). This elevated risk is attributed not only to the high prevalence of pre-existing cardiovascular conditions but also to the additional cardiovascular stress imposed by both ESKD as a condition and the HD procedure itself, such as fluid overload with uncontrolled hypertension (48, 49), hemodynamic instability (50, 51), chronic inflammation (52, 53) and oxidative stress (54), anemia (55), hyperphosphatemia as well as mineral bone disorders (56, 57), and increased circulating β2-microglobulin (β2M) levels (58, 59) (Figure. 2.1).
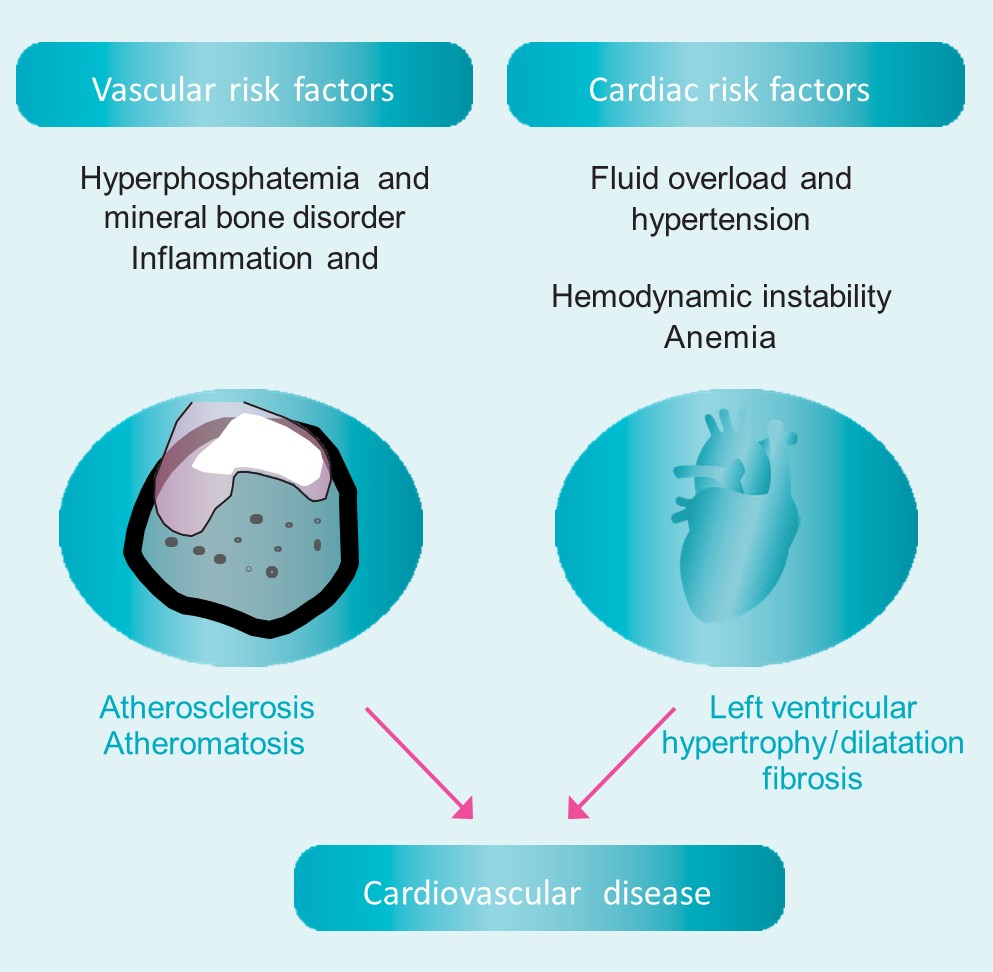
Figure 2.1. | Potential cardiovascular risk factors in dialysis patients.
These compounding factors create a “perfect storm” for the cardiovascular system, explaining why ESKD patients on dialysis face persistently elevated cardiovascular mortality rates despite managing traditional risk factors.
Dialysis modalities differ in the mechanisms by which uremic toxins are removed:
- Conventional HD primarily relies on diffusive clearance through osmotic gradients, concentration gradients generated across a semi-permeable membrane to eliminate small molecular-weight solutes.
- Hemofiltration removes solutes by convection through transmembrane pressure (TMP), which is especially effective in removing middle-molecular-weight (MMW) toxins. Convective clearance combines substitution volume infusion and removal (infusing sterile replacement (substitution) fluid ultrapure dialysate into the circulation at the same rate as it is removed through the dialysis filter, i.e., volume neutral) with ultrafiltration (net removal of fluid from the patient’s circulating blood volume).
- Hemodiafiltration combines diffusive and convective clearances, efficiently removing a broad molecular-weight spectrum of uremic toxins. Indeed, HDF efficiently removes small-molecular-weight uremic solutes (e.g., urea and creatinine) mainly through diffusive transport. Simultaneously, medium-sized uremic molecules (e.g., b2M) are preferentially removed through convective clearance (Figure 2.2).
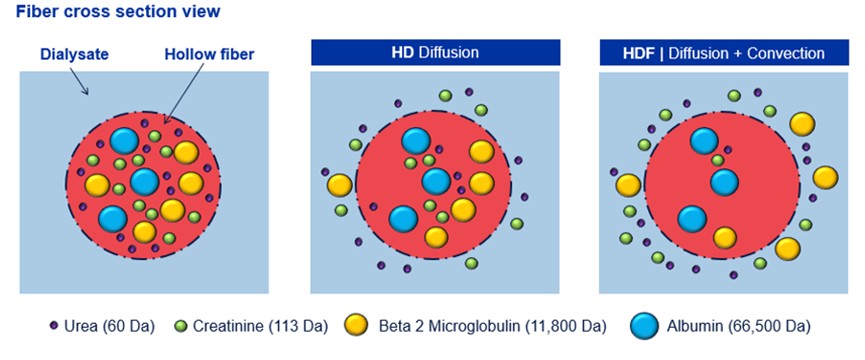
Figure 2.2 | Hemodiafiltration combines diffusion and convection clearances to improve solute removal.
- High-volume HDF achieved by delivering a high convective substitution volume each session maximizes uremic toxin removal. Notably, a large convection volume in HDF is associated with significantly lower mortality: achieving > 23 L of convective clearance per session has been linked to reduced overall and cardiovascular death rates compared to conventional high-flux dialysis (37, 38, 42, 44, 60).
This chapter will present the different dialysis modalities, focusing on the transport of different uremic toxins, with particular emphasis on HDF and its various modalities.
2.2 | Conventional Hemodialysis
Conventional (low- and high-flux) HD is an extracorporeal blood purification technique that leverages the physical and chemical properties of a semi-permeable membrane to achieve solute and fluid exchange between the blood and the dialysate compartments, driven by concentration gradients, pressure gradients, and osmotic forces.
The blood and dialysate flow in opposite directions (counter-current flow) to maximize concentration gradients and enhance diffusion. Conventional HD’s goals are to remove uremic toxins as small solutes (e.g., urea, creatinine) and middle molecules (e.g., β2M), maintain electrolyte homeostasis, restore acid-base balance, and control fluid overload by removing excess plasma water to normalize the extracellular volume and blood pressure.
According to the permeability characteristics of the dialysis membrane, HD can be divided into low-flux and high-flux HD (if low-flux or high-flux hemodialyzers are utilized). These membranes allow selective passage of solutes, rejecting larger components such as proteins and blood cells while allowing small and middle molecules to pass through.
High-flux membranes permit considerably higher amounts of convection in addition to diffusion.
In conventional HD, uremic molecules are removed primarily through diffusive transport, driven by a concentration gradient between the blood (where uremic toxins are at a higher concentration) and the dialysate (where their concentration is lower) across the HD membrane (Figure 2.3).
Smaller molecules diffuse more rapidly than larger ones, as the diffusion rate is inversely related to molecular size. Consequently, HD is particularly effective at clearing smaller solutes, even when larger solutes are small enough to pass through the pores of the dialysis membrane.
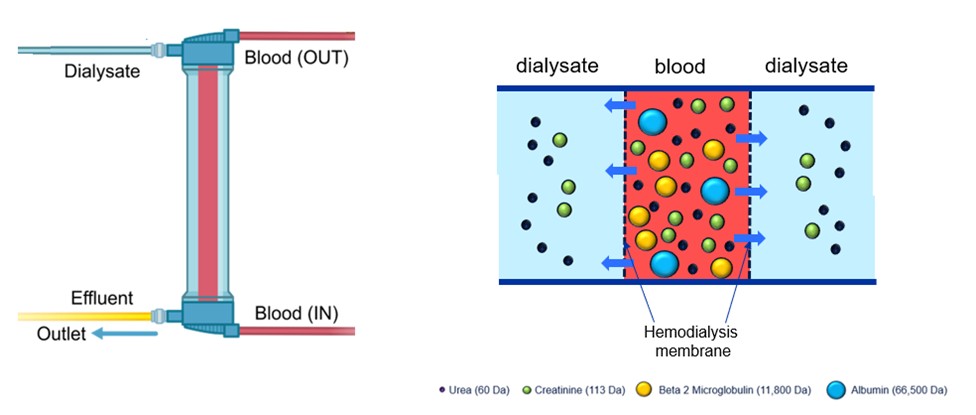
Figure 2.3 | Diffusive transport of uremic molecules in hemodialysis across a dialysis membrane during high-flux hemodialysis.
Fick’s first law governs the rate of diffusion of solutes (Jd, amount of solute transferred per unit time) from the patient’s blood to dialysate across the HD membrane.
Jd = D x A x T x (dc / dx)
D: Diffusivity coefficient of the solute (molecular weight, solubility, electric charge, …)
A: Surface area of the membrane
T: Temperature
dc: Concentration gradient dialysate/blood
dx: Membrane thickness (porosity, pore characteristics, hydrophilicity,…)
2.3 | Hemofiltration (Diafiltration)
In 1967, Henderson et al. introduced the concept of “diafiltration” as a method for removing toxins from blood through a pure convective therapy (61). This approach involved ultrafiltration volumes that exceeded the desired fluid removal, necessitating the infusion of replacement (substitution) fluid to achieve fluid balance and control hydration status and hemodynamic stability. Over time, the term “diafiltration” caused some confusion and was subsequently replaced by the term “hemofiltration” in 1976, as proposed by Burton.
Reliable clinical data on long-term maintenance HF emerged in the early 1970s, with significant contributions from German researchers such as Quellhorst et al. (1, 62). At the time, the widespread recognition of the efficacy of low-flux membranes to clear small molecular weight toxins but not MMW toxins sparked interest in identifying specific “middle molecules” left relatively untouched by conventional low-flux membranes, molecules that might explain the ongoing vicissitudes and complications experienced by patients receiving chronic low-flux HD.
This “middle molecule” hypothesis initially drove a research and development program focused on HF. Even if a particular (or particular class of) offending middle molecule proved elusive, a therapy which nonetheless removed middle molecules “en masse” had obvious therapeutic appeal. However, its clinical application in the late 1970s and 1980s was primarily justified by its stabilizing effect on blood pressure during and between dialysis sessions (17). Patients with cardiovascular comorbidities who regularly experienced hemodynamic instability and discomfort during conventional HD became the initial candidates for HF. HF is a KRT that relies on convective transport to achieve solute clearance.
Unlike traditional HD, predominantly based on diffusion, HF necessitates a highly permeable dialysis membrane capable of facilitating extensive ultrafiltration and solute removal.
To generate sufficient convection, ultrafiltration must be performed at a rate far exceeding the fluid volume required to achieve the patient’s dry weight. Consequently, a substitution fluid is administered to compensate for the ultrafiltered volume, adjusted for the intended weight loss. Convection increases the clearance of middle molecules over that provided by diffusion alone. It is a process where a positive hydrostatic pressure is applied to a fluid, causing it to flow across a semi-permeable membrane.
Solutes are carried with the fluid by “solvent drag“, meaning the fluid pulls the solutes through the membrane, enabling their removal (Figure 2.4), provided the solutes can pass through the membrane pores. Unlike conventional dialysis, HF does not require a dialysis fluid in the classical sense, as the convective transport mechanism drives solute removal (Figure 2.4).
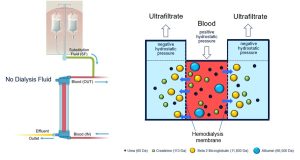
Figure 2.4 | Post-dilution hemofiltration treatment with sterile bags.
The transport dynamics of HF differ substantially from those of HD. Diffusive transport, which dominates in conventional HD, is highly efficient for the clearance of small solutes but becomes increasingly inefficient as molecular weight increases. Specifically, while diffusion effectively removes solutes with molecular weights below 1,000 Daltons (Da), clearance rates decline significantly for larger molecules, such that a 1,000 Da solute is removed at approximately half the rate of a 60 Da solute, like urea. In contrast, convection-based clearance in HF remains effective for larger solutes, making it the preferred mechanism for removing molecules exceeding 2,000–3,000 Da in molecular weight.
The efficiency of convective solute removal is inherently linked to the properties of the dialysis membrane, particularly its sieving characteristics. The mean pore size determines Sieving Coefficient (SC) at the innermost separating region of the membrane, which defines the selective retention or clearance of molecules. The SC for a given molecule and membrane is calculated based on the solute concentration in the fluid after filtration relative to the difference in solute concentration in the fluid (plasma) entering and exiting the dialyzer (SC = 2 CF / CPi + CP0). Solutes that can traverse the membrane’s pores are carried along with the ultrafiltered fluid, making the membrane’s SC a critical determinant of solute clearance. Ideally, the in vivo sieving profile of membranes employed in KRT should closely approximate the physiological sieving curve of the glomerular basement membrane. This ensures optimal removal of both small and larger molecular weight solutes, thereby enhancing the overall efficacy of the treatment.
The clearance achieved in HF is determined by the Ultrafiltration Rate (UFR); UFR is defined as the removal of plasma water and dissolved solutes across the membrane using a pressure gradient, typically controlled by the dialysis machine [UFR = Ultrafiltration coefficient of the membrane multiplied by TMP difference (blood-side pressure minus dialysate-side pressure)].
The membrane’s hydraulic permeability dictates the UFR. To ensure efficient fluid and solute removal, HF requires the use of high-flux membranes with a minimum Ultrafiltration Coefficient (Kuf) of 20 mL/h/mmHg/m². The rate of convection of solute transport (Jd, amount of solute transferred per unit time) from the patient’s blood to dialysate across the HD membrane is calculated by multiplying the UFR, the concentrate of solute (Cs), and the solute sieving coefficient (SC):
Jd = UFR x Cs x SC
UFR: Ultrafiltration rate (volume of plasma water removed per unit time)
Cs: Concentration of the solute in plasma water
SC: Sieving coefficient (fraction of solute passing through the membrane with water)
The magnitude of convective transport, excluding adsorption effects, mainly depends on the UFR, which is influenced by the hydraulic permeability of the membrane’s support region. Convection, therefore, represents the extent to which solutes, determined by their sieving properties at the membrane’s separating region, are transported along with the removed fluid, a process governed by the hydraulic permeability of the membrane wall.
In HF, middle molecules of uremic toxins are removed by maximizing convective transport through extensive UFR beyond the volume required to achieve the patient’s dry weight.
Large substitution fluid volumes are necessary to fully leverage the convective mechanism for physiologically significant blood purification. This is achieved by operating at an optimal UFR relative to the blood flow rates feasible for individual patients, enabling high convective clearances for larger molecular-weight uremic toxins. Typical UFRs in HF are around 25-30% of the blood flow rate and are influenced by the patient’s blood composition and degree of hydration.
From the outset, HF faced significant financial and clinical challenges. The high cost of large volumes of sterile intravenous replacement fluids in pre-packaged bags was not scalable due to manufacturing expense. At the same time, HF alone (in the absence of concomitant dialysate use, as in HD) proved less efficient than HD in clearing low molecular-weight solutes, such as urea and creatinine (Figure 2.5).
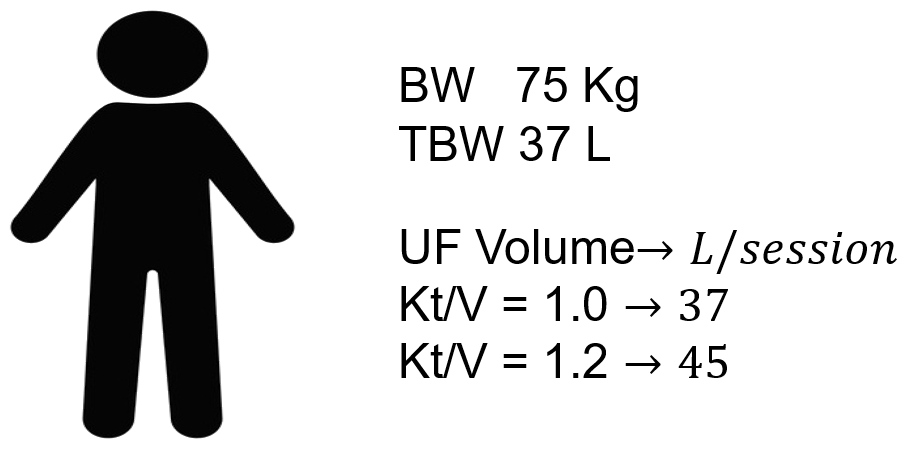
Figure 2.5 | Hemofiltration Kt/V performances and sterile solution consumptions in a patient with body weight (BW) of 75 Kg and 37 L of total body water (TBW).
To counteract the HF-related elevation in systemic urea concentration, longer dialysis times or greater volumes of substitution fluid were required—mainly when administered in pre-dilution mode (i.e., infused into the bloodline prior to passing through the dialysis filter) compared to post-dilution (i.e., infused into the bloodline after passing through the dialysis filter) to enhance convective flux. While improving solute removal, this approach further compounded the financial constraints associated with long-term HF maintenance.
To increase the efficiency of HF in the lower molecular weight range, HF was combined with HD, performed simultaneously, which led to the modality termed hemodiafiltration.
2.4 | Hemodiafiltration
HDF is an advanced dialysis modality that seamlessly integrates the principles of HD and HF within a single treatment session, enhancing both diffusive and convective solute clearance while maintaining patient safety.
HDF was initially performed using bags of sterile substitution fluid in combination with ultrapure dialysate provided by the HD machine. Modern technology utilizes a high-flux hemodialyzer paired with a specially designed dialysis machine that produces sterile substitution fluid in real-time, ensuring safe and efficient therapy delivery and eliminating the need for bags (Figure 2.6). Considering the identified HF limitations outlined above, “online” HDF addresses the challenge of administering very high substitution fluid volumes through online sterile fluid production by the machine, administered directly into the bloodline. In principle, the infusion of online-generated sterile substitution fluid into the closed-loop bloodlines may be pre-dilution or post-dilution. However, most current HDF platforms exploit post-dilution online fluid substitution.
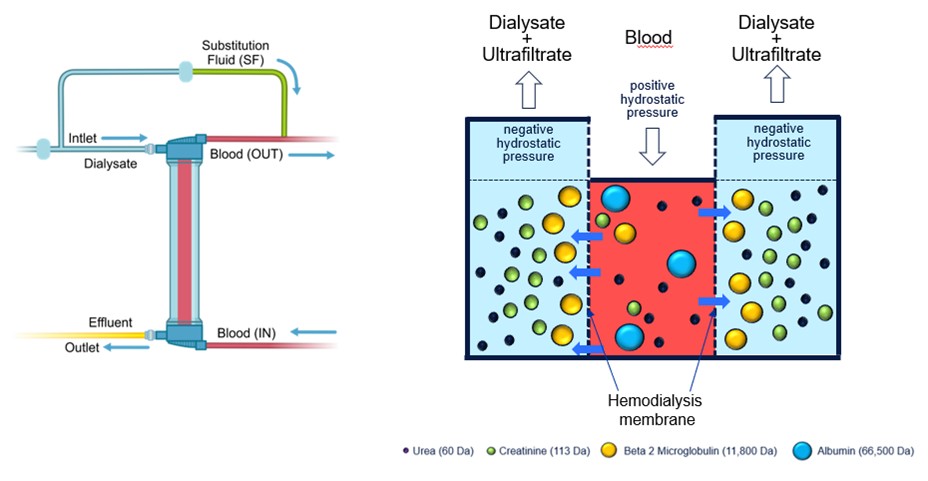
Figure 2.6 | In online post-dilution HDF, the solutes are carried with the fluid by solvent drag in addition to the diffusive transport.
Online HDF combines the diffusive and convective solute removal in a single therapy by ultrafiltering 25-35% of the blood volume processed (Filtration Fraction) using a high-flux hemodialyzer and maintaining fluid balance by infusing online sterile, non-pyrogenic substitution fluid directly into the patient’s blood. Diffusion and enhanced convection enable the removal of both small- and middle-molecular-weight compounds along the UFR solvent drag effect through increased TMP.
Total ultrafiltration exceeds the desired fluid loss to maximize the removal of middle-sized toxins by convection. Therefore, replacement (substitution) fluid must be infused into the extracorporeal circuit at an equal amount minus the desired fluid volume removal to achieve dry weight.
The larger the volume of fluid removed by ultrafiltration (and sub-sequently replaced), the higher the efficiency of HDF.
Although both transport processes occur simultaneously, it is easier to conceptualize the sequence by assuming that diffusion occurs first, followed by the convective removal of the remaining solutes in the blood. For solutes that are effectively cleared by diffusion, such as urea, very little remains available for convective transport. Conversely, solutes not well cleared by diffusion, such as β2M, remain in higher concentrations and are more readily removed by convection. Therefore, combining diffusive and convective transport always results in greater total clearance than using either process alone under the same operational conditions (63, 64) (Figure 2.7).
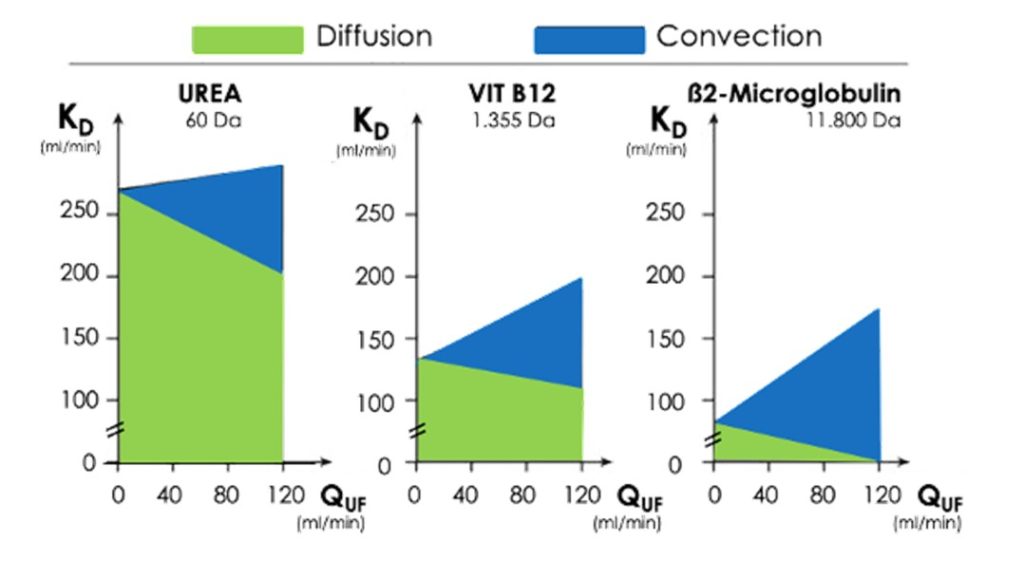
Figure 2.7 | The clearance in HDF of urea, vitamin B12 and b2-microglobulin at increasing ultrafiltration and convective transport (blood flow rate, 300 ml/min; diffusion green, convection blue. QUF = substitution fluid rate/ultrafiltration. Modified from Ledebo (63).
2.5 | Online Hemodiafiltration Modalities
Online HDF treatment modalities can be categorized based upon the point of substitution fluid administration within the extracorporeal circuit into four distinct types: post-dilution HDF, pre-dilution HDF, mixed-dilution HDF and mid-dilution HDF (4, 5). Compared to post-dilution HDF, the dilution factor for pre-dilution HDF is 2, 1.5 for mixed-dilution HDF and mid-dilution HDF. Thus, in pre-, mixed-, and mid-dilution HDF, higher substitution volumes are needed than in post-dilution HDF.
2.5a Post-dilution HDF: Post-dilution HDF is the most commonly used mode of online HDF due to its superior ability to achieve high convective clearances and effective removal of soluble uremic toxins, particularly at normal or elevated blood flow rates.
The substitution fluid is infused downstream of the dialyzer into the venous drip chamber of the extracorporeal circuit (Figure 2.8).
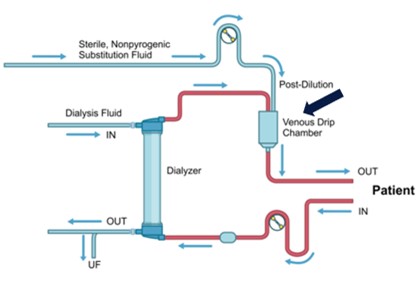
Figure 2.8 | Post-dilution hemodiafiltration.
The high UFR characteristic of post-dilution HDF increases serum protein concentrations as plasma water is removed, leading to a rise in blood viscosity and oncotic pressure. While this facilitates efficient solute removal, it also exposes the membrane to increased hemoconcentration and hyperviscosity.
Consequently, during post-dilution HDF, proteins, such as albumin and globulin, are deposited on the dialysis membrane surface, causing fouling that affects solute removal over time and biocompatibility. This phenomenon necessitates the careful management of filtration parameters.
A key limitation of post-dilution HDF is the restriction on the filtration fraction (FF), which is typically maintained at up to 30% of the blood flow rate. Exceeding this threshold risks hemoconcentration and further increases the likelihood of clot formation and membrane fouling, thereby reducing the efficiency of the treatment.
Despite these challenges, post-dilution HDF remains the preferred modality in clinical practice due to its ability to maximize convective solute clearance while maintaining overall treatment efficacy at higher blood flow rates and reducing the overall water consumption.
Proper optimization of ultrafiltration and substitution parameters is critical to achieving the best therapeutic outcomes in this mode. Therefore, in post-dilution HDF, the degree of convective transport is a critical determinant of overall treatment efficacy.
Several large-scale randomized clinical trials and meta-analyses demonstrated a survival advantage in patients undergoing post-dilution HDF, with convective volumes exceeding 23 liters (HVHDF) (37, 38, 42, 44). Achieving a convective volume of 23 L or more during HDF is a critical factor influencing clinical outcomes. From a clinical standpoint, a delivered convection volume of 23 liters per session, widely recognized as a surrogate marker of the convective dialysis dose, has emerged as a critical threshold associated with improved patient outcomes in HVHDF (37, 38, 42, 44). HVHDF enhances solute clearance, reduces inflammation, and improves survival rates and quality of life, making it a key target in high-efficiency HDF protocols.
2.5b Pre-dilution HDF: The substitution fluid is infused upstream of the dialyzer into the arterial side of the extracorporeal circuit (Figure 2.9). The pre-dilution mode reduces solute concentrations in the blood entering the dialyzer, leading to lower diffusive and convective clearance rates than the post-dilution mode. Despite the reduced solute clearance efficiency, pre-dilution HDF offers several advantages. Decreasing hematocrit and oncotic pressure preserves the TMP gradient along the membrane capillaries. This reduces the risk of clot formation and shear stress, potentially minimizing the formation of a “secondary membrane.”
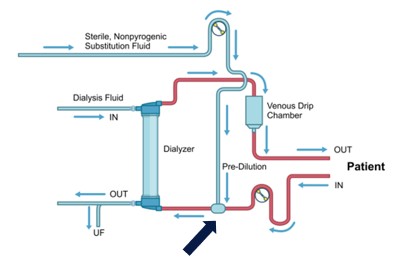
Figure 2.9 | Pre-dilution hemodiafiltration.
Achieving equivalent solute clearances in pre-dilution HDF requires a substitution volume approximately twice as large as that used in post-dilution HDF due to the dilution of solutes entering the hemodialyzer. In Asia-Pacific countries, pre-dilution HDF is widely used, representing 80 to 90% of HDF-treated patients in Japan, where lower blood flow rates are traditionally applied, favoring its use.
2.5c Mixed-dilution HDF. The substitution fluid is infused simultaneously at different rates into the extracorporeal circuit, with approximately 80% delivered upstream (pre-dilution) and 20% downstream (post-dilution) of the dialyzer (Figure 2.10).
Implementing mixed-dilution HDF requires specialized equipment. Specific blood tubing is needed to facilitate the dual infusion of substitution fluid, and a non-standard dialysis machine equipped with an additional pump is necessary to regulate the separate flows for pre- and post-dilution infusion.
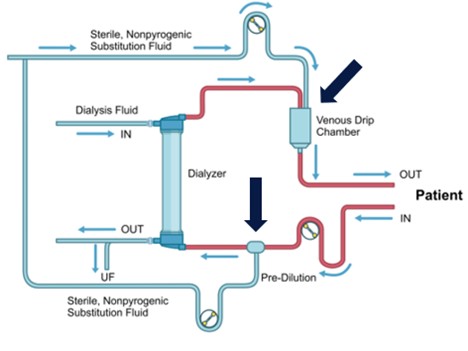
Figure 2.10 | Mixed-dilution hemodiafiltration.
This added complexity limits its widespread adoption. Mixed-dilution HDF represents a sophisticated modality that seeks to balance the strengths of pre- and post-dilution techniques. Optimizing fluid infusion distribution provides effective solute removal while reducing some of the operational challenges associated with other HDF modalities.
2.4d Mid-dilution HDF Mid-dilution HDF is a non-conventional modality that employs a specially designed dialyzer with a unique inlet port for substitution fluid, enabling a combination of pre-dilution and post-dilution modes within the same treatment session (Figure 2.11). This approach leverages the advantages of both dilution strategies while addressing some of their respective limitations.
The dialyzer used in mid-dilution HDF features two distinct high-flux fiber bundles housed within the same unit: an outer annular region and an inner core region. These two compartments are separated by a specially designed header cap, which facilitates the sequential flow of blood and substitution fluid through the dialyzer.
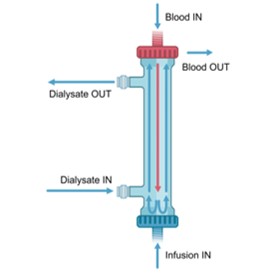
Figure 2.11 | Mid-dilution hemodiafiltration.
Mid-dilution HDF represents an innovative approach to combining the benefits of pre- and post-dilution modalities. However, the complexity of this setup and the requirement for specific dialyzer designs limit its accessibility and widespread application in routine clinical practice.