
Improved Health-Related Quality of Life
Dialysis patients have significantly impaired quality of life (QoL) and a greater prevalence of depressive symptoms compared to the general population, which increases their risks for morbidity and mortality1–3. Intensified HD regimens, as often made more permissible by home therapy, have been shown to address both physical and mental aspects of poor health-related QoL (HRQoL), reduce depressive symptoms, decrease recovery time and improve fatigue after each HD session, and improve sleep quality and adequacy
What do patients have to say about how their lives have been changed by HHD?
Patients and caregivers report the perception that home HD offers them the opportunity to thrive, improves freedom and normality, offers treatment flexibility, and strengthens relationships (Figure 1)6. These positive patient-reported outcomes persist despite the fact that home therapy increases the burden of treatment for patients and their caregivers, with some voicing anxiety about the increased responsibility, fear of self-cannulation and complications, and isolation from medical support. By permitting a greater flexibility in scheduling HD treatment sessions, patients have more freedom to spend time doing the things they like to do – whether spending time with family, engaging in a hobby, or pursuing part-time or full-time employment or education6,7. With less time spent in dialysis facilities and traveling to and from a clinic, patients can participate more in day-to-day household and social activities with friends and family.

Figure 1: Selected quotations from actual patients of positive perceptions, illustrating their perception of how their lives have been changed by HHD (images used are avatars and do not represent the actual patients).6
Several studies have suggested that frequent home HD improves scores on standardized health surveys5. In 2019, Wong and colleagues used the SF-12 Health Survey to compare the HRQoL in patients receiving nocturnal home HD 3-6 nights per week with patients receiving other kidney replacement therapy (KRT) modalities8. They reported that Home HD patients scored 6.7 points higher on the physical component summary, significantly higher than in-center HD patients, but found no concomitant increase in the mental component domain of the SF-12 (Figure 2). While the physical component summary is associated with the physical functioning and limitations caused by physical problems and bodily pain, the mental component summary measures limitations caused by emotional problems, vitality, social functioning, and mental health. Prior to this study, Watanabe and colleagues used the Short Form Health Survey (SF-36 v2) and found that patients using home HD 5-6 times per week during the day for 3-5 hours had higher unadjusted scores in all composite and subscale scores with the exception of general health and mental health composite relative to in-center HD patients dialyzing thrice weekly for 3-5 hours (Figure 2)9.
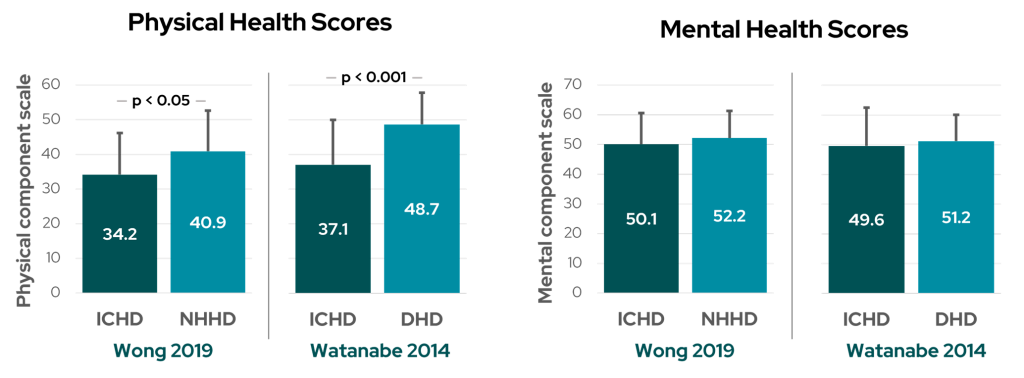
Figure 2: Physical and Mental Health Component Scores from standardized health surveys (Adapted from Wong et al8 and Watanabe et al9). ICHD: in-center hemodialysis; NHHD: nocturnal home hemodialysis; DHD: daily hemodialysis.
In another report, Jaber et al10 surveyed patients from the FREEDOM Study – a multicenter prospective cohort study of short daily HD – and found that after 12 months of dialyzing six times per week, patients had a significant decrease in mean scores on the Beck Depression Inventory (BDI) survey (11.2 vs 7.8, p < 0.001) and the percentage of patients with depressive symptoms (BDI score > 10) significantly decreased (41% vs 27%, p = 0.03).
Finkelstein and colleagues surveyed the same large patient cohort from the FREEDOM study and reported that in the total cohort, the proportion of patients with a mental component summary score of greater than 50 increased from 47% at baseline to 64% after 12 months on frequent HD (Figure 3)11. They also reported an increase in the proportion of participants with a physical component summary score of greater than 50, from 8% at baseline to 24% after 12 months.
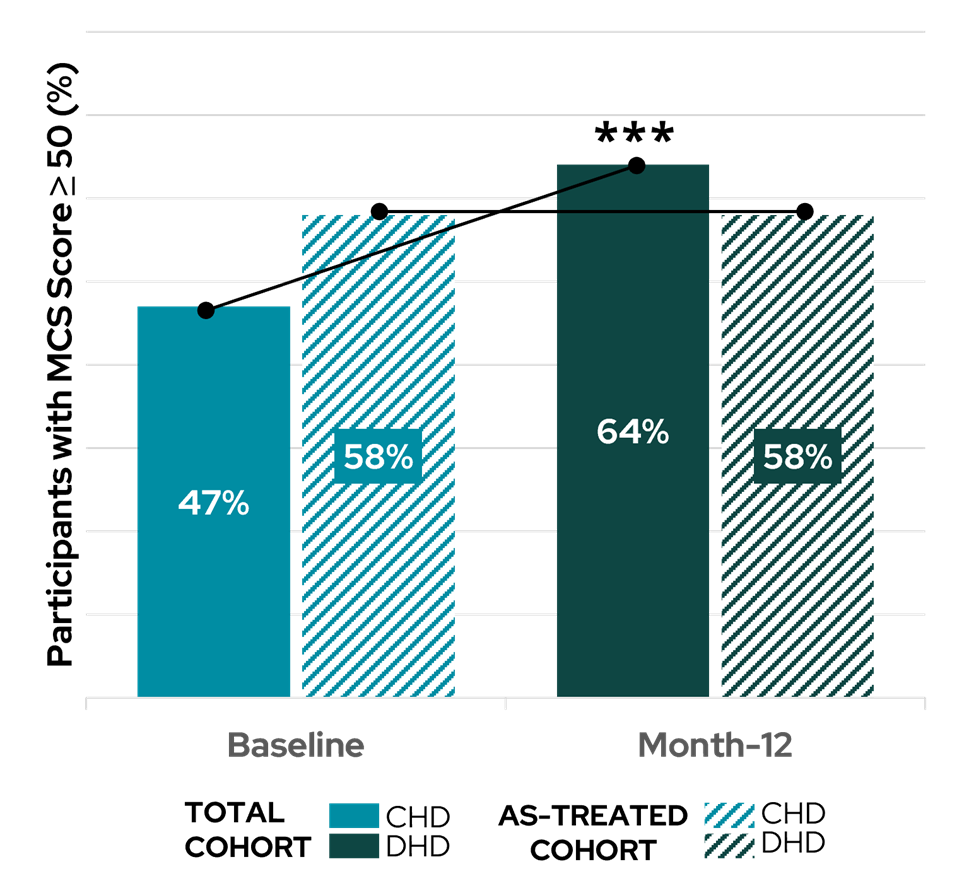
Figure 3: Participants with mental component summary scores of greater than 50 in the total cohort and in the as-treated cohort in patients treated with conventional HD (CHD) and patients treated with short daily HD (DHD) (Adapted from Finkelstein et al11).
Frequent HD is associated with reduced post-dialysis recovery time
In a survey of over 6,500 patients on thrice weekly HD, Rayner et al12 reported a post-dialysis recovery time of over 6 hours in 27% of patients (Figure 4). In the FREEDOM Study, the average recovery time with conventional, thrice weekly HD was 8 hours10. Long recovery time after HD can be a debilitating complication, with each additional hour of recovery time associated with a 5% increased risk of death12. Relative to the majority of patients reporting a 2-6 hour recovery time, HD patients with a 7-12 hour and over 12 hour recovery time have a 22% and 47% increased risk of all-cause mortality, respectively12.
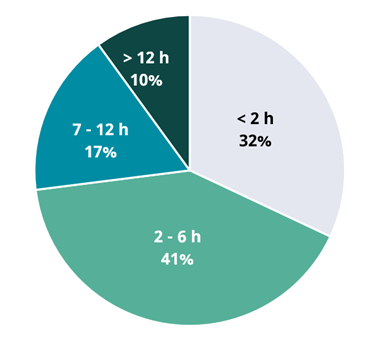
Figure 4: Distribution of Patient-Reported Recovery Times (data from Rayner, et al12).
Increasing the frequency or duration of HD treatment has been shown to reduce recovery time following each dialysis session10,13. Heidenheim and colleagues assessed changes in quality of life in patients enrolled in the London Daily/Nocturnal Hemodialysis Study, after switching from conventional to short daily or long nocturnal HD at home. The authors reported that recovery time decreased dramatically for both groups – as low as 16 minutes for daily HD at the 12-month follow up, and 2 minutes for nocturnal HD at the 15-month follow up – while patients remaining on conventional HD continued to experience post-dialysis recovery durations ranging from 375 to 460 minutes (Figure 5)13. Patients in this study also reported significant declines in fatigue levels in both daily and nocturnal HD groups. Subsequent studies corroborated these findings, with Jaber et al10 reporting an 87% improvement in recovery time with more frequent home HD (476 vs 63 minutes).
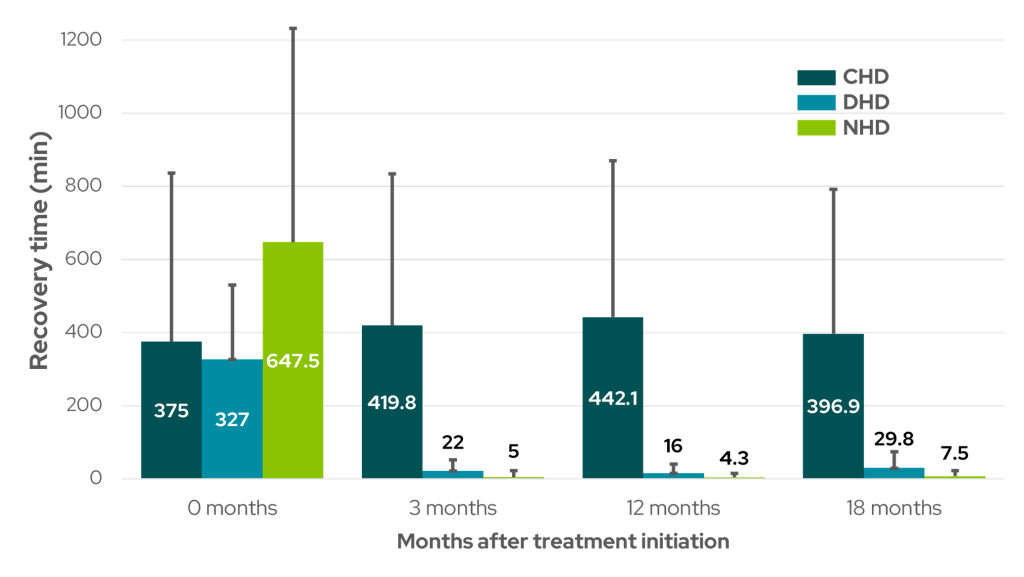
Figure 5: Average amount of time taken to recover after a single dialysis session in patients treating with conventional thrice weekly HD (CHD), short daily HD (DHD), and long nocturnal HD (NHD) at study initiation (0 months) and after 3, 12, and 18-month follow-up (Adapted from Heidenheim et al13).
Frequent HD is associated with improved sleep
Restless legs syndrome (RLS) and sleep disturbances are common in end-stage kidney disease patients and are also associated with increased morbidity and mortality14–18. Restless legs syndrome is characterized by an unpleasant achy or crawly sensation in the legs that is relieved by movement of the affected limb and aggravated by rest14,17. As a result, patients suffer from sleep disturbances, sleep fragmentation, frequent wakening, sleep deprivation, and obstructive sleep apnea. Restless legs syndrome has also been linked with impaired quality of life, increased risk of cardiovascular events, and in patients with severe RLS, a 39% increase in all-cause mortality16,18.
Several studies have reported that more frequent HD is associated with improvement in the prevalence and severity of RLS and sleep disturbances. In 2011, Jaber and colleagues found a significant decrease in patients reporting RLS symptoms from 35% at baseline on conventional thrice weekly in-center HD to 26% 12 months after switching to short daily (6 times weekly) in-center HD (Figure 6)14. The percentage of patients suffering from moderate-to-severe RLS, as measured by the International Restless Legs Syndrome (IRLS) Study Group rating scale (a greater to or equal score of 15), also decreased from 59% to 43% over the same time period (Figure 6)14.
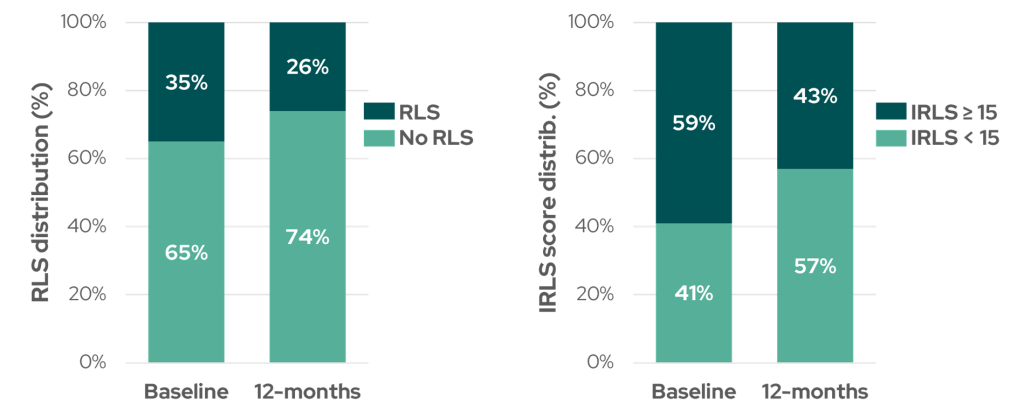
Figure 6: Percentage of study participants with Restless Legs Syndrome (RLS) at baseline and after 12 months of short daily HD (left, p = 0.05), and percentage of patients with moderate-to-severe RLS (defined by IRLS score ≥15) at baseline and after 12 months of short daily HD (right, p = 0.06) (Adapted from Jaber et al14).
Despite limitations in the current data and some studies reporting inconclusive findings, intensified HD regimens have been shown to improve patient perceived health-related QoL, reduce post-dialysis recovery time, and improve the severity of restless leg syndrome and sleep disturbances.
References:
- Valderrábano F, Jofre R, López-Gómez JM. Quality of life in end-stage renal disease patients. American Journal of Kidney Diseases. 2001;38(3):443-464. Available from: https://www.sciencedirect.com/science/article/pii/S0272638601973688.
- Suri RS, Nesrallah GE, Mainra R, et al. Daily hemodialysis: a systematic review. Clin J Am Soc Nephrol. 2006;1(1):33-42. Available from: http://www.ncbi.nlm.nih.gov/pubmed/17699188.
- Walters BAJ, Hays RD, Spritzer KL, Fridman M, Carter WB. Health-related quality of life, depressive symptoms, anemia, and malnutrition at hemodialysis initiation. American Journal of Kidney Diseases. 2002;40(6):1185-1194. Available from: http://www.ncbi.nlm.nih.gov/pubmed/12460037.
- Kraus MA, Kansal S, Copland M, et al. Intensive Hemodialysis and Potential Risks With Increasing Treatment. American Journal of Kidney Diseases. 2016;68(5):S51-S58.
- Bonenkamp AA, van Eck van der Sluijs A, Hoekstra T, et al. Health-Related Quality of Life in Home Dialysis Patients Compared to In-Center Hemodialysis Patients: A Systematic Review and Meta-analysis. Kidney Med. 2020;2(2):139-154.
- Walker RC, Hanson CS, Palmer SC, et al. Patient and Caregiver Perspectives on Home Hemodialysis: A Systematic Review. American Journal of Kidney Diseases. 2015;65(3):451-463.
- Suri RS, Li L, Nesrallah GE. The risk of hospitalization and modality failure with home dialysis. Kidney Int. 2015;88(2):360-368.
- Wong CKH, Chen JY, Fung SKS, et al. Health‐related quality of life and health utility of Chinese patients undergoing nocturnal home haemodialysis in comparison with other modes of dialysis. Nephrology. 2019;24(6):630-637.
- Watanabe Y, Ohno Y, Inoue T, Takane H, Okada H, Suzuki H. Home hemodialysis and conventional in-center hemodialysis in Japan: A comparison of health-related quality of life. Hemodialysis International. 2014;18:S32-S38. Available from: http://doi.wiley.com/10.1111/hdi.12221.
- Jaber BL, Lee Y, Collins AJ, et al. Effect of daily hemodialysis on depressive symptoms and postdialysis recovery time: Interim report from the FREEDOM (Following Rehabilitation, Economics and Everyday-Dialysis Outcome Measurements) Study. American Journal of Kidney Diseases. 2010;56(3):531-539. Available from: https://pubmed.ncbi.nlm.nih.gov/20673601/.
- Finkelstein FO, Schiller B, Daoui R, et al. At-home short daily hemodialysis improves the long-term health-related quality of life. Kidney Int. 2012;82(5):561-569. Available from: http://www.ncbi.nlm.nih.gov/pubmed/22622497.
- Rayner HC, Zepel L, Fuller DS, et al. Recovery time, quality of life, and mortality in hemodialysis patients: the Dialysis Outcomes and Practice Patterns Study (DOPPS). Am J Kidney Dis. 2014;64(1):86-94. Available from: http://linkinghub.elsevier.com/retrieve/pii/S0272638614000316.
- Heidenheim AP, Muirhead N, Moist L, Lindsay RM. Patient quality of life on quotidian hemodialysis. Am J Kidney Dis. 2003;42(1 Suppl):36-41. Available from: http://www.ncbi.nlm.nih.gov/pubmed/12830442.
- Jaber BL, Schiller B, Burkart JM, et al. Impact of Short Daily Hemodialysis on Restless Legs Symptoms and Sleep Disturbances. Clinical Journal of the American Society of Nephrology. 2011;6(5):1049-1056. Available from: https://www.ncbi.nlm.nih.gov/pubmed/21415315.
- Walker S, Fine A, Kryger MH. Sleep complaints are common in a dialysis unit. American Journal of Kidney Diseases. 1995;26(5):751-756.
- Winkelman JW, Chertow GM, Lazarus JM. Restless legs syndrome in end-stage renal disease. Am J Kidney Dis. 1996;28(3):372-378. Available from: https://pubmed.ncbi.nlm.nih.gov/8804235/.
- Nichols DA, Allen RP, Grauke JH, et al. Restless Legs Syndrome Symptoms in Primary Care. Arch Intern Med. 2003;163(19):2323.
- Unruh ML, Levey AS, D’Ambrosio C, Fink NE, Powe NR, Meyer KB. Restless legs symptoms among incident dialysis patients: Association with lower quality of life and shorter survival. American Journal of Kidney Diseases. 2004;43(5):900-909.
GMO-001401 Rev A 11/2024